
Abstract
Introduction
The treatment of type 2 diabetes mellitus (T2DM) continues to pose challenges for clinicians and patients. The dramatic rise in T2DM prevalence, which has paralleled the rise in obesity, has strained the healthcare system and prompted the search for therapies that not only effectively treat hyperglycemia, but are also weight neutral or promote weight loss. In most clinical situations after diagnosis, patients are advised to adopt lifestyle changes and metformin is initiated to help control blood glucose levels. However, metformin may not be tolerated, or may not be sufficient for those with higher glucose levels at diagnosis. Even among those who have initial success with metformin, the majority eventually require one or more additional agents to achieve their treatment goals. Because T2DM is a progressive disease, the requirement for combination treatment escalates over time, driving the need for therapies with complementary mechanisms of action.
Methods and Results
Online public resources were searched using “empagliflozin”, identifying 32 articles in PubMed, and 12 abstracts presented at the 2013 American Diabetes Association meeting. Peer-reviewed articles and abstracts describing preclinical studies and clinical trials were retrieved, and relevant publications included in this review. Trials registered on clinicaltrials.gov were searched for ongoing empagliflozin studies.
Conclusion
The sodium–glucose co-transporter 2 (SGLT2) inhibitors are of great interest since they provide a novel, insulin-independent mechanism of action. The SGLT2 inhibitor empagliflozin has demonstrated promising pharmacodynamic and pharmacokinetic properties. In clinical trials, empagliflozin has demonstrated a good efficacy and safety profile in a broad range of patients with T2DM, and appears to be an attractive adjunct therapeutic option for the treatment of T2DM. Ongoing trials, including patients with T2DM and comorbidities such as hypertension, are expected to provide important additional data, which will further define the role of empagliflozin in a growing movement toward individualized approaches to diabetes care.
Similar content being viewed by others


Introduction
Type 2 diabetes mellitus (T2DM) is a chronic disease characterized by elevated blood glucose levels, insulin resistance, and relative insufficiency of insulin production. The prevalence of T2DM is rising dramatically around the world. For example, in the United States (US) the number of adults with diabetes increased by 75% during the time between a survey conducted during 1988–1994 to a second survey in 2005–2010 [1]. In the US, as elsewhere, this increase is generally seen in parallel with the rise in the prevalence of obesity, which is now at epidemic proportions [1, 2]. The total economic burden associated with diabetes treatment and lost productivity is substantial; in the US alone, these costs have been calculated at 245 billion USD for 2012 [3].
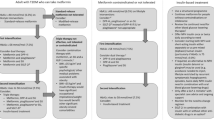
After diagnosis, treatment for T2DM is initially focused on lifestyle management and includes changes in dietary choices, consumption patterns, and the institution of exercise regimens to reduce weight, enhance insulin sensitivity, and lower blood glucose levels [4]. If these strategies do not achieve the desired goals for blood glucose [or if at diagnosis a patient’s glycosylated hemoglobin (HbA1c) level is >7.5%], then guidelines recommend pharmacotherapy at diagnosis [4]. Metformin is recommended as initial therapy with addition of sulfonylureas, thiazolidinediones, dipeptidyl peptidase (DPP)-4 inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, sodium–glucose co-transporter 2 (SGLT2) inhibitors, or insulin as needed [4]. These agents have different mechanisms of action, and different effects on insulin resistance, insulin secretion, and weight. Therefore, the risk/benefit ratio of each drug, or drug combination, needs consideration in light of therapeutic goals and potential safety concerns for individual patients [4].
Of these different classes of anti-diabetes drugs, the SGLT2 inhibitors are the newest. These agents help regulate blood glucose levels by blocking the reuptake of filtered glucose in the proximal tubule, leading to significant excretion of glucose via the urine, which is a novel and insulin-independent approach (Fig. 1) [5]. Clinical experience with SGLT2 inhibitors has increased since the approvals of dapagliflozin [in November 2012 by the European Medicines Agency (EMA) and in January 2014 by the US Food and Drug Administration (FDA)] and canagliflozin (in March 2013 by the FDA and November 2013 by the EMA). A third agent, empagliflozin, is in late-stage clinical trials in a global development program, including the US and Europe. In this review, the available data from these trials, along with preclinical studies, are surveyed to determine the potential value of empagliflozin in the treatment of patients with T2DM.

Key agents and sites of action for type 2 diabetes mellitus drugs. DPP dipeptidyl peptidase, GI gastrointestinal, GIP gastric inhibitory polypeptide, GLP glucagon-like peptide, SGLT2 sodium–glucose co-transporter 2
Review Methods
During November 2013, PubMed (US National Library of Medicine, Bethesda, MD, USA) and the Scientific Sessions Online Resources (American Diabetes Association, Alexandria, VA, USA) were searched using the term “empagliflozin”, identifying 32 articles in PubMed, and 12 clinical abstracts presented at the 2013 American Diabetes Association meeting. Peer-reviewed articles and abstracts describing preclinical studies and clinical trials were retrieved, and relevant publications included in this review. The reference lists of relevant publications were reviewed for potential additional reports. Trials registered on clinicaltrials.gov were searched for ongoing empagliflozin studies, using the search term “empagliflozin” and the criteria “Phase 3”. The analysis in this article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by the author.
Discovery and Brief History of SGLT Inhibitors
For over a century, a naturally occurring botanical glucoside has been known to contribute to glucosuria in animals and humans [6]. This active compound was eventually identified as phlorizin and it was established that increased glucose excretion could help regulate blood glucose levels [6]. Early studies showed that phlorizin inhibited the transport of glucose in a variety of tissues, including the kidney and small intestine [7, 8]. Further investigation identified phlorizin as a competitive inhibitor of the SGLT1 and SGLT2 proteins, which are membrane-embedded proteins responsible for reabsorption of glucose from the glomerular filtrate in the kidney. SGLT1 is also found in the small intestine, where it is responsible for absorption of glucose and galactose.
In a diabetic rat model, phlorizin treatment increased glucose concentration in urine, and normalized plasma glucose levels in the absence of hypoglycemia, in both fasting and fed states [9]. Phlorizin also improved insulin sensitivity [9]. While these properties made phlorizin very interesting, it was ultimately unsuitable for clinical development for several reasons. Firstly, phlorizin is broken down in the gastrointestinal tract, and must thus be administered intravenously; secondly, the active metabolite, phloretin, is a potent inhibitor of facilitative glucose transporters; and thirdly, phlorizin is associated with frequent gastrointestinal adverse events (AEs) including diarrhea and dehydration [10]. Although these events are usually attributed to phlorizin’s limited selectivity for SGLT2 over SGLT1 (and consequent presence of unabsorbed glucose and galactose in the large intestine), early studies with dual SGLT1/2 inhibitors suggest SGLT1 inhibition is not inevitably associated with gastrointestinal AEs [11]. Nevertheless, it was clear that phlorizin was not suitable for further development, but did serve as a basis for the identification of inhibitors with improved safety and tolerability profiles.
Empagliflozin Pharmacological Characteristics and Mechanistic Studies
Extensive drug discovery and development studies in vitro identified BI 10773 (empagliflozin; 1-chloro-4-[β-d-glucopyranos-1-yl]-2-[4-([S]-tetrahydrofuran-3-yl-oxy)-benzyl]-benzene; Fig. 2) as a potent and selective competitive inhibitor of the SGLT2 protein. Empagliflozin is structurally related to phlorizin; however, while phlorizin is an O-glucoside and thus susceptible to degradation by β-glucosidase in the gastrointestinal tract, empagliflozin is a C-glucoside, and the carbon–carbon bond between the glucose and aglycone moieties makes it resistant to gastrointestinal degradation, allowing oral administration [5].

Chemical structure of empagliflozin
The pharmacokinetic and pharmacodynamic (PK/PD) attributes of empagliflozin have been extensively tested in vitro and in vivo, and Table 1 shows key parameters for planned therapeutic doses, 10 mg and 25 mg [12]. Early studies included analysis of cell lines, stably over-expressing human (h) SGLT1, SGLT2, or SGLT4 receptors, which were screened for specific cellular uptake of a radiolabeled test molecule [14C]-alpha-methyl glucopyranoside. In addition, two new cell lines over-expressing hSGLT5 and hSGLT6 were established, and the binding kinetics of [3H]-labeled empagliflozin were also analyzed [13]. Taken together, these studies demonstrated that empagliflozin is a potent inhibitor of hSGLT2, with a half maximal inhibitory concentration (IC50) of 3.1 nM, and has >2,500-fold selectivity for inhibition of SGLT2 versus SGLT1 [13].
Subsequent in vivo pharmacological studies confirmed that empagliflozin lowered blood glucose levels and improved glycemic control in diabetic rodent models, with dose-dependent increases in urinary glucose excretion (UGE) [14]. In addition, 5 weeks of empagliflozin treatment reduced HbA1c levels by 0.3% and 1.1% with 1 or 3 mg/kg, respectively, compared with an increase of 1.1% in vehicle-treated animals. Improved insulin sensitivity was also recorded with empagliflozin [14].
The metabolic response to empagliflozin has been studied in patients with T2DM [15]. As predicted from the theory of glucotoxicity, reduction of blood glucose with empagliflozin was associated with improvements in measures of insulin resistance and beta-cell function. The investigators also observed an unexpected increase in endogenous glucose production, possibly resulting from an increase in plasma glucagon levels [15]. It has been suggested that combination therapy with an agent that inhibits glucagon by increasing incretins (a GLP-1 mimetic or DPP-4 inhibitor) may give synergistic effects for the treatment of hyperglycemia, but this work is still at early stages, and additional studies are needed [16].
Empagliflozin Phase I Studies in Humans: Safety, Tolerability, and Pharmacokinetics
Phase I studies of single doses of empagliflozin were conducted in a study of 72 healthy male volunteers recruited at a single clinic in Germany. Subjects were randomized to an empagliflozin dose of 0.5–800 mg, or placebo [17]. Empagliflozin was quickly absorbed after oral ingestion, with a median time to maximum plasma concentration (t max) of approximately 1.5–2.1 h, and total drug exposures were generally proportional with escalating doses. Empagliflozin also demonstrated a biphasic decline in plasma concentrations during the decay phase, with a terminal elimination half-life ranging from 8.6 to 13.1 h [17].
In these healthy volunteers, the rate of UGE increased with escalating doses, and reached a plateau around the 50-mg dose. The mean total amounts of glucose excreted in the urine during 24 h after administration of empagliflozin (0.5, 2.5, 10, 25, 50, 100, 200, 400, and 800 mg) were 3.1, 30.6, 47.9, 56.5, 63.6, 78.6, 69.1, 90.8, and 61.6 g, respectively, versus 0.06 g with placebo [17]. The amounts of glucose excreted in the urine were similar under fed and fasted conditions, indicating food had no clinically relevant effects on drug absorption. In these healthy volunteers, empagliflozin had a good safety profile and was well tolerated: reported AEs included headaches, nervous system and gastrointestinal disorders; all were reported at similar frequencies in empagliflozin and placebo-treated subjects, and none were dose-dependent. There was one report of hypoglycemia, which was observed 3 h after an oral glucose tolerance test. Since the glucose levels showed mild hypoglycemia (53 mg/dL), it was considered to be reactive hypoglycemia, and therefore not related to study drug [17].
Similar results were seen in another Phase I study of empagliflozin doses ranging from 1 to 100 mg in 48 healthy Japanese men [18]. Empagliflozin was rapidly absorbed in these subjects, with a t max of 1.25–2.50 h, after which plasma concentrations declined with classic biphasic kinetics. Empagliflozin exposures were proportional to doses studied. At the highest doses tested (100 mg), mean UGE was approximately 74 g and UGE was dose-dependent. Empagliflozin was again well tolerated, with no reports of hypoglycemia in any of the subjects [18].
Following these results in healthy volunteers, a study of empagliflozin safety, tolerability, and PK/PD was conducted over 28 days in patients with T2DM [19]. Seventy-eight patients received placebo (n = 16) or empagliflozin once-daily at one of three doses: 10 mg (n = 16), 25 mg (n = 16), or 100 mg (n = 30). Twice as many patients were randomized to the 100-mg safety arm of this study to assess the safety of this high dose of empagliflozin.
Plasma concentrations of empagliflozin were dose-dependent over the full range of doses (10–100 mg) and linear PK were observed [19]. By Day 1, UGE rose from baseline to 74, 90, and 81 g with increasing doses of empagliflozin (10, 25, and 100 mg, respectively). Elevated UGE continued throughout the 28 days of empagliflozin treatment, while virtually no change in UGE was observed with placebo over the same timeframe [19]. Mean daily plasma glucose and fasting plasma glucose (FPG) levels were significantly reduced from baseline in the empagliflozin groups compared with the placebo group [19]. The incidence of AEs was similar, with 50.0, 56.3, and 66.7% of patients in the empagliflozin 10-mg, 25-mg, and 100-mg groups, respectively, experiencing at least one AE versus 62.5% with placebo. The most commonly reported AEs were pollakiuria (10.3%), nasopharyngitis (9.0%), constipation (9.0%), and headache (7.7%) [19].
Additional trials addressing the safety, tolerability, and PK/PD of empagliflozin in patients with either renal or hepatic impairment have recently been reported. An open-label trial grouped 40 patients by estimated glomerular filtration rate to study the impact of renal impairment on the PK/PD profile of a single dose of empagliflozin 50 mg [20]. In patients with renal impairment, peak plasma concentrations of empagliflozin were similar to those with normal renal function. In comparison to patients with normal renal function, total plasma exposure (area under the concentration–time curve from zero to infinity) and the maximum plasma concentration (C max) were modestly increased (Table 2), most likely owing to decreased renal clearance of the drug. Patients with mild or moderate renal impairment had slightly decreased UGE compared with patients with normal renal function; those with severe impairment or renal failure had lower UGE. This suggests that while empagliflozin may be used without dose adjustments in patients with any degree of renal impairment, reductions in plasma glucose levels would be predicted to be less clinically meaningful for those with severe renal impairment [20].
A related open-label clinical trial, also using a single 50-mg dose of empagliflozin, compared 36 patients with various degrees of hepatic impairment: eight each with mild [Child–Pugh class A (5–6 points)], moderate [Child–Pugh class B (7–9 points)], or severe [Child–Pugh class C (10–15 points)] hepatic impairment, and 12 matched controls with normal hepatic function [21]. Use of SGLT2 inhibitors in patients with impaired hepatic function has been an area of potential concern following a case of liver toxicity with dapagliflozin, although after longer follow-up the case was re-classified as auto-immune hepatitis rather than drug-induced liver injury, and data from additional exposure to dapagliflozin have been reassuring [22]. In the empagliflozin study, the drug was rapidly absorbed and after achieving peak concentrations, the expected biphasic decline in plasma drug concentrations was observed [21]. PK parameters were mildly elevated, but were less than twofold the values in patients with normal hepatic function. While ongoing vigilance is always prudent, the study investigators concluded there is no need for adjustment of empagliflozin doses in patients with hepatic impairment [21].
Empagliflozin: Coadministration with Other Drugs and Cardiac Safety
Patients with T2DM vary widely in age and often have significant comorbidities, including advanced cardiovascular disease; therefore, this patient population often is receiving several medications concurrently in addition to other anti-diabetes drugs [23]. Accordingly, any potential adverse interactions between empagliflozin and other commonly prescribed drugs are of clinical interest.
Coadministration with a number of clinically important drugs that could reasonably be expected to be prescribed in the T2DM patient population has been tested in a series of open-label, crossover studies in healthy volunteers. These studies showed that empagliflozin can be given together with the anti-diabetes drugs metformin or sitagliptin, the commonly prescribed cardiovascular drugs verapamil, ramipril, and digoxin, and the anticoagulant warfarin; in each case without the need for dose adjustment for either empagliflozin or the coadministered drug [24–27]. In a similar open-label study, researchers demonstrated a combined oral contraceptive ethinylestradiol 30 μg/levonorgestrel 150 μg once daily can be coadministered with oral empagliflozin 25 mg once daily, without requirement for dose adjustment [28].
A number of drugs are known to prolong the cardiac QT interval, which can lead to life-threatening arrhythmias in treated patients [29]. To assess the cardiac safety of empagliflozin, 30 volunteers with a mean age of 35 years were randomized to a double-blind, placebo-controlled study of single doses of empagliflozin, 25 and 200 mg (therapeutic and supratherapeutic, respectively), versus placebo and open-label moxifloxacin 400 mg as positive control [30]. Within the initial 1–4 h after empagliflozin dosing, the placebo-corrected mean change from baseline in the population heart rate corrected QT interval was 0.6 ms [90% confidence interval (CI) −0.7, 1.9] for empagliflozin 25 mg and −0.2 ms (90% CI −1.4, 0.9) for empagliflozin 200 mg. These values are deemed acceptable since the upper limit of the confidence intervals are <10 ms, which is the International Conference on Harmonization E14 threshold for regulatory concern [31]. Consistent with the results seen in other trials, the tolerability of empagliflozin was good for all study participants, with 23.3% of the empagliflozin group experiencing AEs with empagliflozin compared with 27.6% of the placebo group.
Empagliflozin in Phase II and Phase III Clinical Trials
The favorable data emerging from the various empagliflozin Phase I clinical trials set the stage for subsequent Phase II and Phase III studies in various patient populations. While several trials are ongoing, a number have already been reported in the peer-reviewed literature [32–36].
Phase II Trials
In a Phase II, randomized, double-blind, placebo-controlled clinical trial, the safety, efficacy, tolerability, and PK of empagliflozin were evaluated in patients with T2DM [32]. The investigators randomized 408 patients (treatment-naïve or having completed a 4-week washout) to empagliflozin (5, 10, or 25 mg once daily), placebo, or open-label metformin for 12 weeks. At baseline, the mean ± standard deviation (SD) HbA1c level across all groups was 7.9 ± 0.8%. After 12 weeks, dose-dependent reductions in HbA1c from baseline were seen in the empagliflozin-treated patients (5 mg −0.4%, 10 mg −0.5%, 25 mg −0.6%; p < 0.0001 for all doses vs. placebo +0.1%). Patients in the open-label metformin arm had similar reductions in HbA1c levels of −0.7%, but the metformin arm was not designed to be tested for significance against the double-blind groups [32].
Among the secondary endpoints, FPG levels also decreased with empagliflozin (5 mg −1.29 mmol/L, 10 mg −1.61 mmol/L, 25 mg −1.72 mmol/L; all doses p < 0.0001 vs. placebo +0.04 mmol/L). Of special significance to patients with T2DM, who tend to be either overweight or obese, there were modest but significant decreases in body weight in each of the empagliflozin-treated groups, with changes from baseline of −1.81 kg, −2.33 kg, and −2.03 kg in the 5, 10, and 25-mg groups, respectively (all p < 0.001 vs. placebo); the open-label metformin group had a −1.32 kg decrease versus baseline [32].
The groups had similar rates of AEs, at 32.9% for the placebo group and 29.1% across the empagliflozin groups. Few differences between groups were observed for the most common AEs reported with empagliflozin; these were pollakiuria (3.3% vs. 0% for placebo), thirst (3.3% vs. 0% for placebo), and nasopharyngitis (2.0% vs. 1.2% for placebo) [32]. There were AEs considered consistent with urinary tract infections (UTIs) in 4/244 patients (1.6%) on empagliflozin and 1/82 patients (1.2%) on placebo. Genital infections were reported in five patients (2%) on empagliflozin versus none on placebo. No patients discontinued due to UTIs or genital infections [32].
A second Phase II study was undertaken to evaluate the efficacy and safety of empagliflozin as an add-on therapy to metformin. The investigators randomized 495 patients with T2DM who were inadequately controlled on metformin (HbA1c >7% to ≤10%) to double-blind empagliflozin (1, 5, 10, 25, or 50 mg once daily) or placebo, or to open-label sitagliptin 100 mg once daily, in addition to metformin for 12 weeks [33]. At baseline (while on stable metformin), mean HbA1c across the seven groups ranged from 7.8 to 8.1%. After 12 weeks, mean HbA1c increased by 0.15% in the placebo group, compared with reductions of −0.1%, −0.2%, −0.6%, −0.6%, and −0.5% with empagliflozin 1, 5, 10, 25, or 50 mg, respectively, once daily (all were significant with the exception of 1 mg empagliflozin) [33]. In addition, empagliflozin doses of 5–50 mg significantly reduced FPG levels at 12 weeks, with mean reductions of −2 to −28 mg/dL compared with an increase of 5 mg/dL with placebo (all p < 0.0001). Empagliflozin was also associated with body weight reductions after 12 weeks (−2.3 to −2.9 kg with empagliflozin 5–50 mg vs. −1.2 kg with placebo; p < 0.01) [33].
In this study, empagliflozin was generally well tolerated, and reported frequencies of AEs were similar in the three main treatment groups: empagliflozin (29.6–48.6%), placebo (36.6%), and sitagliptin (35.2%), and the reported rates of hypoglycemia were low and balanced among the groups. The most frequent AEs were UTIs (4.0% vs. 2.8%; empagliflozin vs. placebo) and pollakiuria (2.5% vs. 1.4%; empagliflozin vs. placebo). Genital infections (4.0%) were reported only in the empagliflozin-treated patients [33].
In these Phase II studies, empagliflozin treatment led to dose-dependent, clinically meaningful reductions in HbA1c and FPG, along with concomitant reductions in body weight compared with placebo-treated patients after 12 weeks, indicating empagliflozin can be efficacious as monotherapy or as add-on therapy for patients with T2DM who are not meeting their treatment goals on metformin alone.
Phase III Trials
The Phase III clinical trial program evaluating empagliflozin in patients with T2DM reportedly includes more than 10 multinational trials, between them enrolling more than 14,500 patients, including patients across a wide age range and with a diversity of concomitant diseases [37]. At the time of writing, three Phase III trials have been published in detail, and are reviewed below.
In the first of these Phase III trials, the efficacy and safety of empagliflozin monotherapy was investigated in a randomized, placebo-controlled study of patients with T2DM with HbA1c levels of 7–10% who were treatment-naïve or had not received medication over the 12 weeks preceding the trial [34]. Patients were randomized to empagliflozin 10 mg (n = 224), empagliflozin 25 mg (n = 224), placebo (n = 228), or sitagliptin 100 mg (n = 223) once daily [34]. Patients with HbA1c >10% at screening were not randomized, but were assigned open-label empagliflozin 25 mg for 24 weeks (n = 87).
At 24 weeks, the randomized empagliflozin groups had significant improvements in HbA1c, FPG, and body weight compared with placebo, as shown in Tables 3, 4, and 5 [34]. Furthermore, patients randomized to empagliflozin were more likely to achieve an HbA1c target of <7.0% at week 24: among patients who had HbA1c levels ≥7.0% at baseline, 35% of the empagliflozin 10-mg group and 44% of the 25-mg group achieved HbA1c <7.0% compared with 12% of the placebo group (odds ratio for empagliflozin 10 mg vs. placebo: 4.12; 95% CI 2.44, 6.97; p < 0.0001 and for empagliflozin 25 mg vs. placebo 6.15; 95% CI 3.65, 10.36; p < 0.0001). Both empagliflozin groups also had significant reductions from baseline in systolic blood pressure versus placebo (empagliflozin 10 mg −2.6 mmHg; 95% CI −4.9, −0.4; p = 0.0231; empagliflozin 25 mg −3.4 mmHg; 95% CI −5.7, −1.2; p = 0.0028) [34].
For patients assigned open-label empagliflozin, no formal statistical analyses were performed, but the investigators noted large reductions from baseline to 24 weeks in HbA1c (−3.7%; 95% CI −4.1, −3.3), with 28% of these patients reaching HbA1c <7.0% by week 24. The group also had large reductions in FPG (−4.86 mmol/L; 95% CI −5.55, −4.16), and mean changes in weight (−2.43 kg; 95% CI −3.50, −1.37) and systolic blood pressure (−4.0 mmHg; 95% CI −7.1, −0.9) of a similar level to changes in the empagliflozin 25-mg randomized group.
The majority of AEs were mild, with similar proportions reported in each treatment arm [placebo group, 140 (61%); empagliflozin 10 mg, 123 (55%); empagliflozin 25 mg, 135 (60%); and sitagliptin, 119 (53%)]. Serious AEs also occurred in similar proportions of patients [placebo group, 6 (3%); empagliflozin 10 mg, 8 (4%); empagliflozin 25 mg, 5 (2%); and sitagliptin, 6 (3%)] [34]. The most common AE was hyperglycemia, which was reported in 35 (15%) placebo patients, five (2%) empagliflozin 10-mg patients, four (2%) empagliflozin 25-mg patients, and 13 (6%) sitagliptin patients. The second most common AE was nasopharyngitis, which was reported in 17 (7%) placebo patients, 16 (7%) empagliflozin 10-mg patients, 11 (5%) empagliflozin 25-mg patients, and 15 (7%) sitagliptin patients. Rates of hypoglycemia were <1% in all treatment groups [34]. Laboratory measurements included serum lipids and plasma uric acid concentrations (Tables 6, 7). Of note, empagliflozin appeared to be associated with improvements in uric acid compared with placebo. In addition, compared with placebo, high-density lipoprotein (HDL)-cholesterol increased significantly from baseline in patients treated with empagliflozin 10 or 25 mg, but levels of total cholesterol, low-density lipoprotein (LDL)-cholesterol, or triglycerides did not change [34].
The safety and efficacy of empagliflozin as add-on therapy in patients with T2DM receiving metformin with or without a sulfonylurea was assessed in a randomized, double-blind Phase III trial; two sub-studies were defined by the patients’ background medication at screening. In the first part of the study, patients on metformin only were randomized to 24 weeks of double-blind treatment with either empagliflozin 10 mg (n = 217) or 25 mg (n = 213) once daily or placebo (n = 207) [38]. As with the previous trial, patients with HbA1c >10% at screening were not randomized, and instead were included in an open-label empagliflozin 25-mg arm (n = 69).
Preliminary results have been presented, and support the use of empagliflozin as add-on treatment to metformin, with the empagliflozin groups having significant improvements in HbA1c, FPG, and body weight compared with placebo after 24 weeks (Tables 3, 4, 5) [38]. Among patients who had HbA1c levels ≥7.0% at baseline, 13% of the placebo group achieved an HbA1c <7.0% by 24 weeks compared with 38% of the empagliflozin 10-mg group (odds ratio, 4.72; p < 0.001 vs. placebo) and 39% of the empagliflozin 25-mg group (odds ratio, 4.67; p < 0.001 vs. placebo). Of note, a weight loss of >5% of body weight was achieved by 4.8% of patients in the placebo arm after 24 weeks, compared with 21.2% on empagliflozin 10 mg, and 23.0% on empagliflozin 25 mg [38]. The empagliflozin groups also had significant reductions in systolic blood pressure, with mean changes of −4.5 ± 0.7 mmHg in the 10-mg group and −5.2 ± 0.7 mmHg in the 25-mg group.
For the group of patients with very high HbA1c at screening, who were assigned open-label empagliflozin 25 mg in addition to their background metformin, HbA1c fell by a mean ± standard error (SE) of −3.2 ± 0.2% from a baseline mean of 11.1 ± 0.2%. Improvement was also seen in FPG, with a mean ± SE reduction of −3.02 ± 0.57 mmol/L, from a baseline mean of 11.30 ± 0.43 mmol/L. The group also had reductions from baseline in body weight (mean ± SE −1.91 ± 0.59 kg) and systolic blood pressure (mean ± SE −2.4 ± 1.6).
In this trial, AEs were reported by 57.1%, 49.5%, and 58.7% of patients on empagliflozin 10 mg, empagliflozin 25 mg, and placebo, respectively. Hypoglycemia (defined as plasma glucose ≤70 mg/dL, and/or requiring assistance) was reported in very low proportions of patients (1.8% in the empagliflozin 10-mg arm, 1.4% in the empagliflozin 25-mg arm, and 0.5% in the placebo arm), and none of the cases required assistance [38]. AEs consistent with UTIs were reported in low proportions across the treatment arms (5.1%, 5.6%, and 4.9% in the empagliflozin 10-mg, 25-mg, and placebo arms, respectively). Rates of AEs associated with genital infection were also low with empagliflozin, but appeared more frequent than with placebo (3.7% and 4.7% in the 10-mg and 25-mg empagliflozin arms vs. none in patients receiving placebo) [38].
In the second part of the study, patients with HbA1c inadequately controlled on metformin and a sulfonylurea were randomized to add on once-daily empagliflozin 10 mg (n = 225), empagliflozin 25 mg (n = 216), or placebo (n = 225) for 24 weeks [35]. Improvements were seen in glycemic control, with reductions in HbA1c levels after 24 weeks being significantly greater in the empagliflozin-treated groups, as were reductions in FPG and body weight, as shown in Tables 3, 4, and 5 [35]. Patients were more likely to achieve HbA1c <7.0% with empagliflozin, with 26.3% of the empagliflozin 10-mg group reaching this goal (odds ratio vs. placebo 3.85; 95% CI 2.17, 6.85; p < 0.001) and 32.2% in the empagliflozin 25-mg group (odds ratio vs. placebo 5.22; 95% CI 2.95, 9.24; p < 0.001). The effects of 24 weeks of empagliflozin on body weight (Table 5) were consistent with earlier reports, with significant differences in the adjusted means for empagliflozin versus placebo [35]. Reductions in blood pressure were of a similar level to those seen with empagliflozin used as monotherapy, with a placebo-corrected reduction in the empagliflozin 10-mg group of −2.7 mmHg (95% CI −4.6, −0.8; p = 0.005) and in the 25-mg group of −2.1 (95% CI −4.0, −0.2; p = 0.032).
In this study, 101 patients with HbA1c >10% at screening were treated with open-label empagliflozin 25 mg as add-on to stable metformin and sulfonylurea. The mean ± SE change from baseline in HbA1c at week 24 was −2.9 ± 0.2%, and the mean value fell from 11.2 ± 1.3% at baseline to 8.2 ± 0.1% at week 24. At week 24, the mean ± SE change from baseline in FPG was −3.02 ± 0.37 mmol/L, change in body weight was −1.76 ± 0.40 kg, and change in systolic blood pressure was −4.3 ± 1.2 mmHg.
AEs were reported at similar proportions across treatment groups, at 67.9% in the empagliflozin 10-mg group, 64.1% in the empagliflozin 25-mg group, and 62.7% in the placebo group [35]. Events consistent with UTIs were reported in 10.3% and 8.3% of the empagliflozin 10-mg and 25-mg groups, respectively, versus 8.0% of the placebo group, while events consistent with genital infections were reported in 2.7% and 2.3% of the respective empagliflozin groups versus 0.9% of the placebo group [35]. For LDL-cholesterol and triglycerides, there were no significant differences compared with placebo, while there was a small increase in HDL-cholesterol (Table 6). In the randomized empagliflozin groups, there were small decreases in uric acid (Table 7).
The third Phase III trial published is a randomized, double-blind, placebo-controlled trial that examined the efficacy and safety of empagliflozin in patients with T2DM who were on pioglitazone at screening; patients could also be receiving metformin [36]. Patients were randomized and treated with once-daily empagliflozin 10 mg (n = 165), 25 mg (n = 168), or placebo (n = 165) for 24 weeks [36]. Unlike the aforementioned trials, the design of this study did not include an open-label arm for patients with very high HbA1c at screening.
The investigators found that 24 weeks of empagliflozin treatment resulted in significant reductions in HbA1c and FPG (Tables 3, 4), and more patients with HbA1c ≥7.0% at baseline achieved HbA1c <7.0% with empagliflozin 10 mg (23.8%) and 25 mg (30.0%) than with placebo (7.7%) (odds ratio for empagliflozin 10 mg vs. placebo: 3.85; 95% CI 1.88, 7.92; p < 0.001; odds ratio for empagliflozin 25 mg vs. placebo: 5.02; 95% CI 2.49, 10.12; p < 0.001). Empagliflozin was also associated with significant reductions in body weight (Table 5) and larger proportions of patients experienced reduction of >5% of body weight (18.8% and 13.7% of patients receiving 10 mg and 25 mg of empagliflozin, compared with 5.5% of patients receiving placebo). Empagliflozin was also associated with reductions in blood pressure compared with placebo: systolic blood pressure fell by −3.9 mmHg (95% CI −6.23, −1.50; p = 0.001) with empagliflozin 10 mg and −4.7 mmHg (95% CI −7.08, −2.37; p < 0.001) with empagliflozin 25 mg [36].
In this study, as in previous studies, empagliflozin was well tolerated and the incidence of AEs was not significantly different from placebo. Similar rates of AEs were reported in all three treatment arms (67.3%, 71.4%, and 72.7% of patients in the 10-mg, 25-mg, and placebo groups, respectively). Rates of reported hypoglycemia (plasma glucose ≤70 mg/dL and/or requiring assistance) were also similar across treatment arms (1.2%, 2.4%, and 1.8% of the respective groups), and no patient required assistance. The proportion of patients with AEs related to UTIs was similar across groups (17.0%, 11.9%, and 16.4% of patients on 10 mg, 25 mg, and placebo, respectively); events consistent with genital infection were seen more commonly with empagliflozin (8.5%, 3.6%, and 2.4% of patients on 10 mg, 25 mg, and placebo, respectively); however, all were mild or moderate in intensity and none led to premature study discontinuation [36]. Measurement of serum lipids showed significant increase in HDL-cholesterol in the empagliflozin 10-mg group, but a non-significant increase in the 25-mg group (Table 6). No significant differences were reported for total cholesterol, LDL-cholesterol, or triglycerides in either of the empagliflozin treatment arms (Table 6). Again, small decreases were seen in uric acid levels with empagliflozin, of approximately the same level seen in the study of empagliflozin as add-on to metformin plus sulfonylurea (Table 7).
Anticipated Results: Recently Completed or Ongoing Clinical Trials
The clinical development program for empagliflozin is at a relatively advanced stage; nonetheless, further Phase II and Phase III studies are either recently completed or in progress, and additional Phase III trials registered on the US National Institutes of Health registry at ClinicalTrials.gov are shown in Table 8 [43–49]. Given the number of options available for treatment of T2DM, empagliflozin will need to be assessed as add-on therapy to insulin, among other agents, as well as in initial combination therapies. The Phase III studies reported above were placebo-controlled, but to draw definite conclusions regarding comparative efficacy, an active-controlled study is required, and a 4-year Phase III trial of empagliflozin versus glimepiride is underway [39]. Studies are also required to investigate blood pressure profiles in hypertensive patients, as well as effects in patients with renal impairment, and studies in these groups have reported preliminary data [40, 41]. The empagliflozin Phase III program also includes a cardiovascular outcome event trial, enrolling approximately 7,000 patients at high cardiovascular risk [42]. Japanese regulatory authorities also require a range of trials in Japanese patients, and these are underway. Clearly, the number of clinical trials that are expected to report in the near future will provide a wealth of data on the safety and efficacy of empagliflozin treatment, to help optimize treatment regimens for individual patients.
Conclusions
Based on the evidence available to date, empagliflozin appears to have a promising pharmacologic profile. Pharmacodynamic and pharmacokinetic characteristics include: (1) very high selectivity for the SGLT2 over SGLT1 receptors, potentially minimizing off-target effects; (2) predictable pharmacokinetics, and no known drug–drug interactions with other drugs commonly prescribed for this patient population; (3) favorable pharmacodynamics, including additive control of plasma glucose levels via inhibition of reuptake in the kidney, with a well-defined dose–response relationship; (4) a good safety profile, with no increase in hypoglycemia compared with placebo; and (5) acceptable tolerability in all patient populations studied to date. The most common AEs reported to date include nasopharyngitis, UTIs, and genital tract infections. Changes in uric acid and LDL-cholesterol are of considerable interest—while the changes in uric acid appear favorable, the changes in lipid profiles have been less consistent between studies—yet it must be remembered that these values were captured as safety endpoints in the trials, and thus any potential benefit cannot be defined without further studies specifically comparing these endpoints.
The addition of the SGLT2 inhibitors, with their novel and insulin-independent mechanism of action, to the collection of available anti-diabetes therapies has a number of implications for the clinical management of diabetes. These include: (1) enhanced glycemic control, without undue concerns with regard to the development of hypoglycemia in treated patients; (2) a novel, insulin-independent treatment option for patients who have been receiving insulin secretagogues for an extended period of time, and may be experiencing diminished responsiveness to these agents due to beta-cell fatigue; (3) the ability to use these drugs in patients who have significant co-morbidities, including appropriate ranges of renal and hepatic impairment without dose-adjustment; and (4) the co-administration of the SGLT2 inhibitors in patients who are currently receiving commonly prescribed medications including antihypertensive agents, anti-clotting agents, and oral contraceptives, all without clinically meaningful changes in the dosing of any of these drugs.
Additional Phase II and Phase III trials are underway and have been designed to test the safety and efficacy of empagliflozin over longer follow-up and in larger numbers of patients, representing a broad range of clinical subtypes (severity, duration, age, ethnicity, etc.). These ongoing trials will provide key data on the safety and efficacy of empagliflozin, often in combination with other anti-diabetes treatments, including cardiovascular outcomes data in patients at high cardiovascular risk. Therefore, patients and their healthcare providers will be in an informed position to leverage the potential of these drugs, in the context of a growing movement toward more individualized approaches to diabetes care.
References
Cheng YJ, Imperatore G, Geiss LS, Wang J, Saydah SH, Cowie CC, et al. Secular changes in the age-specific prevalence of diabetes among US adults: 1988–2010. Diabetes Care. 2013;36(9):2690–6.
Sherwin R, Jastreboff AM. Year in diabetes 2012: the diabetes tsunami. J Clin Endocrinol Metab. 2012;97(12):4293–301.
American Diabetes Association. Economic costs of diabetes in the US in 2012. Diabetes Care. 2013;36(4):1033–46.
Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, Bush MA, et al. AACE comprehensive diabetes management algorithm 2013. Endocr Pract. 2013;19(2):327–36.
Nair S, Wilding JP. Sodium glucose cotransporter 2 inhibitors as a new treatment for diabetes mellitus. J Clin Endocrinol Metab. 2010;95(1):34–42.
Ehrenkranz JR, Lewis NG, Kahn CR, Roth J. Phlorizin: a review. Diabetes Metab Res Rev. 2005;21(1):31–8.
Kleinzeller A, Kolínská J, Benes I. Transport of monosaccharides in kidney-cortex cells. Biochem J. 1967;104(3):852–60.
Alvarado F, Crane RK. Phlorizin as a competitive inhibitor of the active transport of sugars by hamster small intestine, in vitro. Biochim Biophys Acta. 1962;56:170–2.
Rossetti L, Smith D, Shulman GI, Papachristou D, DeFronzo RA. Correction of hyperglycemia with phlorizin normalizes tissue sensitivity to insulin in diabetic rats. J Clin Invest. 1987;79(5):1510–5.
Abdul-Ghani MA, Norton L, Defronzo RA. Role of sodium-glucose cotransporter 2 (SGLT 2) inhibitors in the treatment of type 2 diabetes. Endocr Rev. 2011;32(4):515–31.
Zambrowicz B, Freiman J, Brown PM, Frazier KS, Turnage A, Bronner J, et al. LX4211, a dual SGLT1/SGLT2 inhibitor, improved glycemic control in patients with type 2 diabetes in a randomized, placebo-controlled trial. Clin Pharmacol Ther. 2012;92(2):158–69.
Heise T, Seman L, Macha S, Jones P, Marquart A, Pinnetti S, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of multiple rising doses of empagliflozin in patients with type 2 diabetes mellitus. Diabetes Ther. 2013;4(2):331–45.
Grempler R, Thomas L, Eckhardt M, Himmelsbach F, Sauer A, Sharp DE, et al. Empagliflozin, a novel selective sodium glucose cotransporter-2 (SGLT-2) inhibitor: characterisation and comparison with other SGLT-2 inhibitors. Diabetes Obes Metab. 2012;14(1):83–90.
Thomas L, Grempler R, Eckhardt M, Himmelsbach F, Sauer A, Klein T, et al. Long-term treatment with empagliflozin, a novel, potent and selective SGLT-2 inhibitor, improves glycaemic control and features of metabolic syndrome in diabetic rats. Diabetes Obes Metab. 2012;14(1):94–6.
Ferrannini E, Muscelli E, Frascerra S, Baldi S, Mari A, Heise T, et al. Metabolic response to sodium-glucose cotransporter 2 inhibition in type 2 diabetic patients. J Clin Invest. 2014;124(2):499–508.
Merovci A, Solis-Herrera C, Daniele G, Eldor R, Fiorentino TV, Tripathy D, et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J Clin Invest. 2014;124(2):509–14.
Seman L, Macha S, Nehmiz G, Simons G, Ren B, Pinnetti S, et al. Empagliflozin (BI 10773), a potent and selective SGLT2 inhibitor, induces dose-dependent glucosuria in healthy subjects. Clin Pharmacol Drug Dev. 2013;2:152–61.
Sarashina A, Koiwai K, Seman LJ, Yamamura N, Taniguchi A, Negishi T, et al. Safety, tolerability, pharmacokinetics and pharmacodynamics of single doses of empagliflozin, a sodium glucose cotransporter 2 (SGLT 2) inhibitor, in healthy Japanese subjects. Drug Metab Pharmacokinet. 2013;28(3):213–9.
Heise T, Seewaldt-Becker E, Macha S, Hantel S, Pinnetti S, Seman L, et al. Safety, tolerability, pharmacokinetics and pharmacodynamics following 4 weeks’ treatment with empagliflozin once daily in patients with type 2 diabetes. Diabetes Obes Metab. 2013;15(7):613–21.
Macha S, Mattheus M, Halabi A, Pinnetti S, Woerle HJ, Broedl UC. Pharmacokinetics, pharmacodynamics and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, in subjects with renal impairment. Diabetes Obes Metab. 2014;16(3):215–22.
Macha S, Rose P, Mattheus M, Cinca R, Pinnetti S, Broedl UC, et al. Pharmacokinetics, safety and tolerability of empagliflozin, a sodium glucose cotransporter 2 inhibitor, in patients with hepatic impairment. Diabetes Obes Metab. 2013 (Epub ahead of print).
Center for Drug Evaluation and Research. 2014. Summary review. Available at http://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/202293Orig1s000SumR.pdf. Accessed February 21 2014.
Standards of medical care in diabetes-2014. Diabetes Care. 2014;37(Suppl 1):S14–80.
Macha S, Dieterich S, Mattheus M, Seman LJ, Broedl UC, Woerle HJ. Pharmacokinetics of empagliflozin, a sodium glucose cotransporter-2 (SGLT2) inhibitor, and metformin following co-administration in healthy volunteers. Int J Clin Pharmacol Ther. 2013;51(2):132–40.
Brand T, Macha S, Mattheus M, Pinnetti S, Woerle HJ. Pharmacokinetics of empagliflozin, a sodium glucose cotransporter-2 (SGLT-2) inhibitor, coadministered with sitagliptin in healthy volunteers. Adv Ther. 2012;29(10):889–99.
Macha S, Sennewald R, Rose P, Schoene K, Pinnetti S, Woerle HJ, et al. Lack of clinically relevant drug–drug interaction between empagliflozin, a sodium glucose cotransporter 2 inhibitor, and verapamil, ramipril, or digoxin in healthy volunteers. Clin Ther. 2013;35(3):226–35.
Macha S, Rose P, Mattheus M, Pinnetti S, Woerle HJ. Lack of drug–drug interaction between empagliflozin, a sodium glucose cotransporter 2 inhibitor, and warfarin in healthy volunteers. Diabetes Obes Metab. 2013;15(4):316–23.
Macha S, Mattheus M, Pinnetti S, Woerle HJ, Broedl UC. Effect of empagliflozin on the steady-state pharmacokinetics of ethinylestradiol and levonorgestrel in healthy female volunteers. Clin Drug Investig. 2013;33(5):351–7.
van Noord C, Eijgelsheim M, Stricker BH. Drug- and non-drug-associated QT interval prolongation. Br J Clin Pharmacol. 2010;70(1):16–23.
Ring A, Brand T, Macha S, Breithaupt-Groegler K, Simons G, Walter B, et al. The sodium glucose cotransporter 2 inhibitor empagliflozin does not prolong QT interval in a thorough QT (TQT) study. Cardiovasc Diabetol. 2013;12(1):70.
Food and Drug Administration, US Department of Health and Human Services. Guidance for industry: E14 clinical evaluation of QT/QTc interval prolongation and proarrhythmic potential for non-antiarrhythmic drugs. Rockville, MD, 2005.
Ferrannini E, Seman L, Seewaldt-Becker E, Hantel S, Pinnetti S, Woerle HJ. A Phase IIb, randomized, placebo-controlled study of the SGLT2 inhibitor empagliflozin in patients with type 2 diabetes. Diabetes Obes Metab. 2013;15(8):721–8.
Rosenstock J, Seman LJ, Jelaska A, Hantel S, Pinnetti S, Hach T, et al. Efficacy and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, as add-on to metformin in type 2 diabetes with mild hyperglycaemia. Diabetes Obes Metab. 2013;15(12):1154–60.
Roden M, Weng J, Eilbracht J, Delafont B, Kim G, Woerle HJ, et al. Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2013;1(3):208–19.
Häring HU, Merker L, Seewaldt-Becker E, Weimer M, Meinicke T, Woerle HJ, et al. Empagliflozin as add-on to metformin plus sulfonylurea in patients with type 2 diabetes: a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care. 2013;36(11):3396–404.
Kovacs CS, Seshiah V, Swallow R, Jones R, Rattunde H, Woerle HJ, et al. Empagliflozin improves glycaemic and weight control as add-on therapy to pioglitazone or pioglitazone plus metformin in patients with type 2 diabetes: a 24-week, randomized, placebo-controlled trial. Diabetes Obes Metab. 2013 (Epub ahead of print).
Boehringer Ingelheim. Phase III data show investigational compound empagliflozin reduced blood glucose in adults with type 2 diabetes treated with basal insulin. 2013. Available at https://www.boehringer-ingelheim.com/news/news_releases/press_releases/2013/22_june_2013_empagliflozin2.html. Accessed February 17 2013.
Häring H-U, Merker L, Seewaldt-Becker E, Weimer M, Meinicke T, Broedl UC, et al. Empagliflozin as add-on to metformin for 24 weeks improves glycemic control in patients with type 2 diabetes (T2DM) [abstract 1092-P]. Diabetes. 2013;62(Suppl 1):A282.
Ridderstråle M, Svaerd R, Zeller C, Kim G, Woerle HJ, Broedl UC. Rationale, design and baseline characteristics of a 4-year (208-week) phase III trial of empagliflozin, an SGLT2 inhibitor, versus glimepiride as add-on to metformin in patients with type 2 diabetes mellitus with insufficient glycemic control. Cardiovasc Diabetol. 2013;12:129.
Barnett AH, Mithal A, Manassie J, Jones R, Rattunde H, Woerle HJ, et al. Empagliflozin in patients with type 2 diabetes mellitus (T2DM) and renal impairment (RI) [abstract 1104-P]. Diabetes. 2013;62(Suppl 1):A286.
Tikkanen I, Narko K, Zeller C, Green A, Salsali A, Broedl UC, et al. Empagliflozin improves blood pressure in patients with type 2 diabetes (T2DM) and hypertension [abstract 942]. Diabetologia. 2013;56(Suppl 1):S377.
Inzucchi SE, Zinman B, Lachin JM, Wanner C, Ferrari R, Bluhmki E, et al. Design of the empagliflozin cardiovascular outcome event trial in type 2 diabetes mellitus [abstract 944]. Diabetologia. 2013;56(Suppl 1):S378.
NCT01306214. Safety and efficacy of BI 10773 as add-on to insulin regimen in patients with type 2 diabetes mellitus. 2014. Available at http://clinicaltrials.gov/show/NCT01306214. Accessed March 15 2014.
NCT01984606. Efficacy and safety of empagliflozin versus sitagliptin in patients with type 2 diabetes. 2014. Available at http://clinicaltrials.gov/ct2/show/NCT01984606?term=NCT01984606&rank=1. Accessed March 15 2014.
NCT01719003. Safety and efficacy study of empagliflozin and metformin for 24 weeks in treatment-naive patients with type 2 diabetes. 2014. Available at http://clinicaltrials.gov/ct2/show/NCT01719003?term=NCT01719003&rank=1. Accessed March 15 2014.
NCT01778049. Linagliptin as add-on therapy to empagliflozin 10 mg or 25 mg with background metformin in patients with type 2 diabetes. 2014. Available at http://clinicaltrials.gov/ct2/show/NCT01778049?term=NCT01778049&rank=1. Accessed March 15 2014.
NCT01422876. Efficacy and safety of empagliflozin/linagliptin fixed-dose combination in treatment-naïve and metformin-treated type 2 diabetes patients. 2014. Available at http://clinicaltrials.gov/ct2/show/NCT01422876?term=NCT01422876&rank=1. Accessed March 15 2014.
NCT01734785. Safety and efficacy of the combination of empagliflozin and linagliptin compared to linagliptin alone over 24 weeks in patients with type 2 diabetes. 2014. Available at http://clinicaltrials.gov/ct2/show/NCT01734785?term=NCT01734785&rank=1. Accessed March 15 2014.
NCT01368081. Empagliflozin comprehensive add-on study in Japanese subjects with type 2 diabetes mellitus. 2014. Available at http://clinicaltrials.gov/ct2/show/NCT01368081?term=NCT01368081&rank=1. Accessed March 15 2014.
Acknowledgments
The author meets the ICMJE criteria for authorship for this manuscript, takes responsibility for the integrity of the work as a whole, and has given final approval for the version to be published. Boehringer Ingelheim funded article processing charges for this review. Medical writing assistance, supported financially by Boehringer Ingelheim, was provided by José L. Walewski, Ph.D. (Envision Scientific Solutions, Southport, CT, USA). Boehringer Ingelheim was given the opportunity to check the data used in the manuscript for factual accuracy only.
Conflict of interest
Janet B. McGill is a consultant/advisor for Boehringer Ingelheim, Lilly, Abbott, Merck, Janssen, Mannkind, McNeil, Sanofi, and NovoNordisk. Research grants were received from Novartis, Mannkind, Sanofi, Takeda, Andromeda, and Pfizer.
Compliance with ethics
The analysis in this article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article
Cite this article
McGill, J.B. The SGLT2 Inhibitor Empagliflozin for the Treatment of Type 2 Diabetes Mellitus: a Bench to Bedside Review. Diabetes Ther 5, 43–63 (2014). https://doi.org/10.1007/s13300-014-0063-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-014-0063-1