
Abstract
Introduction
The timeline between a decision made and delivery of the baby is termed decision delivery interval (DDI). According to current recommendations, an emergency caesarean section must be performed within 30 min of the decision. The present study was conducted with an objective to assess DDI in a busy obstetric unit in India and its impact on obstetric outcome.
Material and Method
A total of 480 women with indications of category I (emergency): Immediate threat to life of woman or foetus (n = 66), and category II (urgent): Maternal or foetal compromise but not immediately life-threatening (n = 414), were studied in the context of DDI and composite adverse perinatal outcomes including fresh stillbirth, 5-min Apgar score <7 and NICU admission.
Result
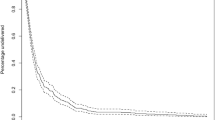
Recommended DDI of <30 min could be achieved in 30% cases of emergency CS only. Sixty-three per cent with prolapsed cord could be delivered within 30 min. The composite neonatal outcomes were not significantly increased up to DDI of 60 min for category I (emergency) (except in prolapsed cord) and up to 90 min in category II (urgent) caesarean sections.
Conclusion
Authors propose reconsideration of the present recommendations of DDI in categories I and II, while Crash CS (cord prolapse or catastrophic antepartum haemorrhage) should be a separate group with recommended DDI of 30 min. For the remaining cases in the present emergency CS group, the suggested DDI of 60 and, for urgent group, 90 min may be made following further studies to prevent this DDI yardstick from becoming a rod at our back.

Similar content being viewed by others


References
Royal College of Obstetricians and Gynaecologists. Classification of urgency of caesarean section—a continuum of risk (Good Practice No. 11). London: RCOG Press; 2010.
Clinical negligence scheme for trusts clinical risk management standards for Acute Trusts Level 3 Assessment of Barts and the London NHS Trust 22nd and 23rd November 2010.
Bloom SL, Leveno KJ, Spong CY, et al. Decision-to-incision times and maternal and infant outcomes. Obstet Gynecol. 2006;108:6–11.
Cerbinskaite A, Malone S, McDermott J, et al. Emergency caesarean section: influences on the decision-to-delivery interval. J Pregnancy. Volume 2011, Article ID 640379, doi:10.1155/2011/640379.
Kei-Man CHOW, Shui-Lam MAK. Maternal and fetal outcomes in extremely urgent caesarean delivery in relation to the decision-to delivery interval. Hong Kong J Gynaecol Obstet Midwifery. 2015;15(1):16–22.
Chukwudi OE, Okonkwo CA. Decision—delivery interval and perinatal outcome of emergency caesarean sections at a tertiary institution. Pak J Med Sci. 2014;30(5):946–50.
Oppong SA, Tuuli MG, Seffah JD, et al. Is there a safe limit of delay for emergency caesarean section in ghana? results of analysis of early perinatal outcome. Ghana Med J. 2014;48(1):24–30.
Amankwah Y, Walker M. A prospective study of the efficiency of the “code 333” process at the Ottawa hospital. JOGC. 2011;33(3):244–51.
Umar UA, Gaya SA. Outcome of umbilical cord prolapse at Aminu Kano Teaching Hospital, Kano, North-Western Nigeria. Niger J Basic Clin Sci. 2015;12:20–4.
Leung TY, Chung PW, Rogers MS, et al. Urgent caesarean delivery for fetal bradycardia. Obstet Gynecol. 2009;14:1023–8.
Rotich SK, Ndavi MP, Rukaria-Kaumbutho R, et al. Early perinatal outcome in cases delivered through Caesarean section following clinical diagnosis of severe foetal distress at Kenyatta National Hospital. East Afr Med J. 2006;83:250–8.
Roy KK, Baruah J, Kumar S, et al. Cesarean section for suspected fetal distress, continuous fetal heart monitoring and decision to delivery time. Indian J Pediatr. 2008;75:1249–52.
Bloom SL, Leveno KJ, Spong CY, et al. Decision-to-incision times and maternal and infant outcomes. Obstet Gynecol. 2006;108:6–11.
Pearson GA, Kelly B, Russell R, et al. Target decision to delivery intervals for emergency caesarean section based on neonatal outcomes and three year follow-up. Eur J Obstet Gynecol Reprod Biol. 2011;159(2):276–81.
Kolas T, Hofos D, Olan P. Predictions for the decision to-delivery interval for emergency Caesarean section in Norway. Acta Obstetricia et Gynecologica. 2006;85:561–6.
Singh R, Deo S, Pradeep Y. The decision-to-delivery interval in emergency Caesarean sections and its correlation with perinatal outcome: evidence from 204 deliveries in a developing country. Trop Doct. 2012;42(2):67–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that there is no conflict of interest.
Ethical approval
All procedures followed were in accordance with ethical standard of the responsible committee on human experiments (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008(5). This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Nalini Mishra is MD, DGO, DNB (O&G), MNAMS, FICOG and is currently working as Professor, Dept of O&G, Govt Med College, Chhattisgarh, India. Ruchi Gupta MD, Associate Professor, Dept of O&G, Govt Med College, Chhattisgarh, India. Nomita Singh MBBS, Resident Surgical Officer, Dept of O&G, Govt Med College, Chhattisgarh, India.
Rights and permissions
About this article

Cite this article
Mishra, N., Gupta, R. & Singh, N. Decision Delivery Interval in Emergency and Urgent Caesarean Sections: Need to Reconsider the Recommendations?. J Obstet Gynecol India 68, 20–26 (2018). https://doi.org/10.1007/s13224-017-0991-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-017-0991-6