
Abstract
Aim of the present study
To assess the changes in hormonal profile (serum FSH, LH, prolactin and total testosterone) following laparoscopic ovarian drilling (LOD) in patients with polycystic ovarian syndrome.
Materials and methods
Fifty patients with PCOS have been included in this study. Serum prolactin, total testosterone, follicular-stimulating hormone (FSH) and luteinizing hormone (LH) levels have been used as biochemical markers, before and after procedures.
Results
Laparoscopic ovarian drilling was successfully employed without any surgical complications and on an average follow-up time of 24 weeks after the procedure. During the follow-up serum values for prolactin, total testosterone and LH have decreased significantly and FSH levels remained unchanged after the procedure.
Conclusions
The LOD in patients with PCOS may avoid or reduce the risk of OHSS and the multiple pregnancy rate induced by gonadotropin therapy. The high pregnancy rate and the economic aspect of the procedure offer an attractive management for patients with PCOS. However, LOD can be considered as second-line treatment after clomiphene citrate treatment failure and/or resistance.
Similar content being viewed by others


Introduction
Polycystic ovarian syndrome (PCOS) is a common endocrinal disorder affecting 5–10 % of the women in reproductive age; it is characterized by chronic anovulation, biochemical and/or clinical evidence of hyperandrogenism and enlarged polycystic ovaries [1].
At the joint consensus meeting of the American Society for Reproductive Medicine and the European Society of Human Reproduction and Embryology (ASRM/ESHRE) a refined definition of the PCOS was agreed, namely the presence of two out of the following three criteria [2]:
-
Oligo- and/or anovulation.
-
Hyperandrogenism (clinical and/or biochemical).
-
Polycystic ovaries.
***With the exclusion of other etiologies.
New evidence-based steps in treating PCOS
Currently, we have three ESHRE/ASRM PCOS consensus workshops [3–5]:
-
1.
First (Rotterdam, 2003; criteria and diagnosis).
-
2.
Second (Thessaloniki, 2007; evidence-based treatment).
-
3.
Third (Amsterdam, 2010; women’s health aspects of PCOS).
-
The latest evidence-based protocols for treatment of PCOS according to second ESHRE/ASRM PCOS consensus workshop (Thessaloniki, 2007; evidence-based treatment):
-
Emphasis on importance of lifestyle modifications.
-
Use of aromatase inhibitors versus CC for ovulation induction.
-
Letrozole appears to improve live birth rate and pregnancy rate in PCOS, compared to CC [6].
-
Double-blind, multicenter trial, 750 randomized letrozole or clomiphene citrate for up to five cycles. Letrozole had higher live birth/ovulation rates without significant differences in overall congenital anomalies [7].
-
-
Use of metformin in PCOS should be restricted to patients with glucose intolerance [guidelines issued by ESHRE/ASRM regarding the induction of ovulation with metformin in PCOS require reconsideration (top 10 articles since 2013)] [8].
-
Second-line intervention includes either exogenous gonadotropins or LOD. Exogenous gonadotropin is highly effective, but risk of multiple pregnancies (careful monitoring is must) [11].
-
Recommended third-line treatment is in vitro fertilization (IVF) [12].
-
-
The aim of the present study was to determine the effectiveness of laparoscopic ovarian drilling on endocrine parameters for sub-fertile women with clomiphene resistant polycystic ovarian syndrome.
Patients and Methods
This study is a prospective interventional study. It was conducted at Zagazig University Hospital, Obstetrics and Gynecology Department, Endoscopy Unit, from January 2014 to June 2015. It was carried out on 50 patients suffering from polycystic ovarian disease, who attended the Endoscopic and Infertility Clinic of Zagazig University Hospital. They were candidate for laparoscopic ovarian drilling.
-
The inclusion criteria will include:
-
All patients are in the reproductive age group. (age between 19 and 36 years).
-
Patients were diagnosed as PCOS on the basis of the following criteria:
(ESHRE/ASRM, Rotterdam Consensus Workshop Group [3]) (presence of two out of the following three criteria):
-
Menstrual disturbances (oligo- or amenorrhea)
-
Clinical and/or biochemical signs of hyperandrogenism
-
Typical ultrasonographic findings of polycystic ovaries.
-
So PCO patients will be diagnosed:
-
1.
Clinically (as hirsutism, acne, obesity, oligo- or amenorrhea).
-
2.
Trans-vaginal ultrasonography (in which there is at least one ovary contains 10 follicles between 2 and 8 mm in diameter in one plane, arranged either peripherally around a dense core of ovarian stroma or scattered throughout an increased amount of stroma).
-
3.
By hormonal profile (in which there is increased androgen, LH and decreased FSH, and LH-to-FSH ratio more than 2.5).
-
Normal hysterosalpingogram (HSG) of patient and normal semen analysis of her husband.
-
All patients were previously initiated for ovulation induction by clomiphene citrate, for six cycles.
-
-
The exclusion criteria will include:
-
Absence of inclusion criteria or patient’s refusal.
-
Any patient with other causes of hyperandrogenism such as congenital adrenal hyperplasia, androgen-secreting tumors or Cushing’s syndrome.
-
Absolute contraindication to laparoscopy.
-
Pregnancy.
-
Patients who receive any drugs that may increase serum prolactin level as sedatives, anti-emetics and anti-histaminics.
-
Male factors of infertility.
-
Other causes of infertility other than anovulatory PCOS: as tubal factor of infertility.
-
Methods (Steps of performance):
All patients had undergone the following:
-
thorough history taking, including:
-
Personal history.
-
Menstrual history (LMP, inter menstrual pain or discharge, regularity of cycles, amount, age of menarche).
-
Obstetric history (parity, mode of delivery if patient got pregnant before and type of infertility).
-
History of the present illness (type & duration of infertility, symptoms of hyperandrogenism, galactorrhea, menopausal symptoms and any investigations done).
-
Family history.
-
Contraceptive history.
-
Past history (deliveries, drugs, operations)
-
-
Complete physical examination.
-
General examination (BMI, measure waist/hip ratio, presence of hirsutism).
-
Abdominal and local examination.
-
-
Measurement of body mass index by the following equation:
$$ {\text{BMI}} = \frac{{{\text{weight}}\, \left( {\text{Kg}} \right)}}{{{\text{Height}}^{2}\,({\text{M }}^{2} )}} $$
Preoperative
-
1.
Baseline blood samples were obtained before operation in all patients to asses serum levels of (FSH, LH, prolactin and total testosterone) with the following precautions:
-
At afternoon, to exclude diurnal variation of prolactin.
-
At rest.
-
No intercourse in the preceding night.
-
2–3 days after the commencement of spontaneous or progesterone induced menstrual bleeding.
-
-
2.
The samples were labeled; sera were separated and frozen until the end of the study and were assayed by the same kit of radioimmunoassay (RIA).
-
3.
This step had been performed at Laboratory Unit, Zagazig University Hospital.
Operation
After the fulfillment of inclusion and exclusion criteria, the patients were randomized for either unilateral or bilateral laparoscopic ovarian drilling.
The technique of LOD used in our hospital: Briefly, a specially designed a diathermy probe was used to penetrate deep in the ovarian stroma at four points with the aid of a short burst of diathermy at 40 W for 4 s.
Postoperative (24 weeks after operation)
Blood sample was taken from each patient after 24 weeks from the operation, to compare preoperative and postoperative hormonal changes after laparoscopic ovarian drilling.
Laboratory analysis had been performed at Laboratory Unit, Zagazig University Hospital.
Results
The studied patients demographically were categorized (Table 1).
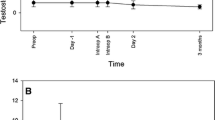
Hormonal profile of the participants has been documented before and after LOD as shown in Fig. 1 and Table 2.

Hormonal changes after laparoscopic ovarian drilling
We noticed that there was a significant decrease in serum LH levels from (14.84 ± 4.37) before drilling to (6.06 ± 1.52) after drilling. We noticed that there was insignificant change in serum FSH levels from (6.59 ± 1.08) before drilling to (6.43 ± 0.91) after drilling.
There was a significant change in LH-to-FSH ratio from (2.31 ± 0.77) before drilling to (0.95 ± 0.23) after drilling.
There was a significant decrease in serum prolactin levels from (27.12 ± 37.56) before drilling to (14.82 ± 5.15) after drilling.
There was a significant decrease in serum total testosterone levels from (2.05 ± 0.48) before drilling to (0.85 ± 0.31) after drilling.
Discussion
Laparoscopic ovarian drilling (LOD) is one mode of surgical therapy used for inducing ovulation, and it is associated with less trauma and fewer postoperative adhesions [13].
LOD can be considered as second-line therapy in all cases that do not respond in 6-month time to clomiphene citrate therapy [14].
Many studies tried to predict the ovulatory response to LOD in patients with clomiphene citrate resistant PCOS. The study of Van wely et al. [15] was a multivariable analysis done on 38 patients using clinical, ultrasonographic and endocrinal parameters to predict the failure of ovulation within 8 weeks after electrocautery. They revealed that women who were younger at menarche (<13 years), and had a lower LH-to-FSH ratio (<2) and a lower glucose level (<4.5 mmol/l), were not likely to benefit from LOD.
Hayashi et al. [16] found that the preoperative luteinizing hormone level is the most important predictive factor in diagnosis of PCOS, and they stated that LOD for patients with low preoperative LH levels (<7.5 IU/l) is not only ineffective, but also may impair ovarian reserve.
-
The changes that we had found in our study in the level of LH, LH-to-FSH ratio and total testosterone are in agreement with that of Felemban et al.; Cleemann et al.; Api et al.; Kandil and Selim; Mustafa and Tulay; Demirturk et al.; Godinjak and Javorić; Abuelghar et al. [17–24].
-
The decrease in serum prolactin after LOD that we had found in our study comes in consistence with those studies done by Alborzi; Alborzi et al.; Kriplani et al. [25–27].
-
Our results in serum prolactin level after LOD come in contrast to the study done by Gjönnaess et al.; Mustafa and Tulay [21, 28] who observed that there were no differences between the endocrine assays of prolactin concentration in all patients after LOD. This may be due to: They did their study on patients with normal prolactin levels before LOD.
-
And also come in contrast to the study done by Al-Ojaimi; Parsanezhad et al.; Hendriks et al. [29–31] who observed elevation in serum prolactin level after LOD. This may be due to:
-
The short period of follow-up (only 4 weeks after LOD).
-
LOD technique was different as they used three punctures with only 20 W for 2 s in drilling.
-
-
In our present study we could not find any significant changes in the mean levels of FSH after LOD. These results are in agreement with Felemban et al.; Takeuchi et al.; Mustafa and Tulay; Abuelghar et al. [17, 21, 24, 32].
-
In contrast to our finding Api et al.; Demirturk et al.; Godinjak and Javorić [19, 22, 23] reported a significant rise of FSH level after laparoscopic ovarian drilling through long duration of follow-up. This may be due to:
-
Long duration of follow-up may be more than 1 year.
-
They had conducted their studies on different age group, different patient number and different patient criteria.
-
Different technique of LOD.
-
Conclusion
-
We conclude that we could assert that laparoscopic ovarian drilling can improve the hormonal profile of patients with polycystic ovarian disease.
-
Laparoscopic ovarian drilling reduces LH, LH-to-FSH ratio, prolactin and testosterone levels in patient with PCOS.
-
These changes may help in inducing ovulation and avoiding OHSS.
References
Goodarzi MO, Dumesic DA, Chazenbalk G, et al. Polycyctic ovary syndrome: etiology, pathogenesis and diagnosis. Nat Rev Endocrinol. 2011;7:219–31.
Fauser B, Tarlatz B, Chang J. The Rotterdam ESHRE/ASRM-sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long term health risks related to polycystic ovary syndrome. Hum Reprod. 2004;19:41–7.
ESHRE/ASRM, Rotterdam Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2003;81:19–25.
Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Consensus on infertility treatment related to polycystic ovary syndrome. Fertil Steril. 2008;89(3):505–22.
Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Consensus on women’s health aspects of polycystic ovary syndrome (PCOS). Hum Reprod. 2012;27(1):14–24.
Franik S, Kremer JA, Nelen WL, et al. Aromatase inhibitors for subfertile women with polycystic ovary syndrome: summary of a Cochrane review. Fertil Steril. 2015;103(2):353–5.
Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med. 2014;371(2):119–29.
Panidis D, Tziomalos K, Papadakis E, et al. The guidelines issued by the European Society for Human Reproduction and Embryology and the American Society for Reproductive Medicine regarding the induction of ovulation with metformin in patients with the polycystic ovary syndrome potentially require reconsideration. Horm (Athens). 2013;12(2):192–200.
Ayaz A, Alwan Y, Farooq MU. Efficacy of combined metformin-clomiphene citrate in comparison with clomiphene citrate alone in infertile women with polycystic ovarian syndrome (PCOS). J Med Life. 2013;6(2):199–201.
Tso LO, Costello MF, Albuquerque LE, et al. Metformin treatment before and during IVF or ICSI in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2014;11:CD006105.
Moazami Goudarzi Z, Fallahzadeh H, Aflatoonian A, et al. Laparoscopic ovarian electrocautery versus gonadotropin therapy in infertile women with clomiphene citrate-resistant polycystic ovary syndrome: a systematic review and meta-analysis. Iran J Reprod Med. 2014;12(8):531–8.
Wan HL, Hui PW, Li HW, et al. Obstetric outcomes in women with polycystic ovary syndrome and isolated polycystic ovaries undergoing in vitro fertilization: a retrospective cohort analysis. J Matern Fetal Neonatal Med. 2015;28(4):475–8.
Farquhar C, Brown J, Marjoribanks J. Laparoscopic, “drilling” by diathermy or laser for ovulation induction in anovulatory polycystic ovary syndrome. Cochrane Database Syst Rev. 2012;6:CD001122.
Ghobadi C, Nguyen TH, Lennard MS, et al. Evaluation of an existing nomogram for predicting the response to clomiphene citrate. Fertil Steril. 2007;87(3):597–602.
Van Wely M, Bayram N, Van der Veen F, et al. Predictors for treatment failure after laparoscopic electrocautery of the ovaries in women with clomiphene citrate resistant polycystic ovary syndrome. Human Reprod. 2005;20(4):900–5.
Hayashi H, Ezaki K, Endo H, et al. Preoperative luteinizing hormone levels predict the ovulatory response to laparoscopic ovarian drilling in patients with clomiphene citrate-resistant polycystic ovary syndrome. Gynecol Endocrinol. 2005;21(6):307–11.
Felemban A, Tan SL, Tulandi T. Laparoscopic treatment of polycystic ovaries with insulated needle cautery: a reappraisal. Fertil Steril. 2000;73(2):266–9.
Cleemann L, Lauszus FF, Trolle B. Laparoscopic ovarian drilling as first line of treatment in infertile women with polycystic ovary syndrome. Gynecol Endocrinol. 2004;18(3):138–43.
Api M, Gorgen H, Cetin A. laparoscopic ovarian drilling in polycystic ovary syndrome. Eur J Obstet Gynecol Reprod Biol. 2005;199:76–81.
Kandil M, Selim M. Hormonal and sonographic assessment of ovarian reserve before and after laparoscopic ovarian drilling in polycystic ovary syndrome. BJOG. 2005;112(10):1427–30.
Mustafa K, Tulay K. Hormonal profiles and clinical outcome after laparoscopic ovarian drilling in women with polycystic ovarian syndrome. Med Sci Monit. 2005;11(1):29–34.
Demirturk F, Caliskan AC, Aytan H, et al. Effects of ovarian drilling in middle Black Sea region Turkish women with polycystic ovary syndrome having normal and high body mass indices. J Obstet Gynaecol Res. 2006;32(5):507–12.
Godinjak Z, Javorić R. Clinical outcome and hormone profiles before and after laparoscopic electroincision of the ovaries in women with polycystic ovary syndrome. Bosn J Basic Med Sci. 2007;7(2):171–5.
Abuelghar WM, Bayoumy HA, Ellaithy MI, et al. Women with clomiphene citrate resistant polycystic ovarian disease: predictors of spontaneous ovulation after laparoscopic ovarian drilling. Eur J Obstet Gynecol Reprod Biol. 2014;175:178–85.
Alborzi S. Laparoscopic ovarian cauterization in patients with polycystic ovaries; clinical outcome and endocrine changes. Iran J Med Sci. 1994;19:120–4.
Alborzi S, Khodaee R, Parsanejad ME. Ovarian size and response to laparoscopic ovarian electro-cauterization in polycystic ovarian disease. Int J Gynaecol Obstet. 2001;74(3):269–74.
Kriplani A, Manchanda R, Agarwal N, et al. Laparoscopic ovarian drilling in clomiphene citrate-resistant women with polycystic ovary syndrome. J Am Assoc Gynecol Laparosc. 2001;8(4):511–8.
Gjönnaess A. Late endocrine effects of ovarian electrocautery in women with polycystic ovary syndrome. Fertil Steril. 1998;69(4):697–701.
Al-Ojaimi EH. Endocrine changes after laparoscopic ovarian drilling in clomiphene citrate-resistant women with polycystic ovarian syndrome. Saudi Med J. 2004;25(8):1032–9.
Parsanezhad ME, Alborzi S, Zolghadri J, et al. Hyperprolactinemia after laparoscopic ovarian drilling: an unknown phenomenon. Reprod Biol Endocrinol. 2005;3:31.
Hendriks ML, Ket JC, Hompes PG, et al. Why does ovarian surgery in PCOS help? Insight into the endocrine implications of ovarian surgery for ovulation induction in polycystic ovary syndrome. Hum Reprod Update. 2007;13(3):249–64.
Takeuchi S, Futamura N, Takubo S, et al. Polycystic ovary syndrome treated with laparoscopic ovarian drilling with a harmonic scalpel. A prospective randomized study. J Reprod Med. 2002;47(10):816–20.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All of authors report no conflict of interest and no financial benefits related to this article.
Ethical approval
All procedures performed in our study involving human participants were in accordance with the ethical standards of the institutional review board (IRB), Zagazig University, Egypt. (IRB Approval No.:1427/28-4-2014)
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Elsayed A. Elnaggar (M.D) is professor of Obstetrics and Gynecology in Department of Obstetrics and Gynecology at Zagazig University Hospital, Egypt, and Head of Endoscopic Unit in Obstetrics and Gynecology Department at Zagazig University Hospital; Youssef Abo Elwan (M.D) is professor of Obstetrics and Gynecology in Department of Obstetrics and Gynecology at Zagazig University Hospital, Egypt; Safaa A. Ibrahim (M.D) is assistant professor of Obstetrics and Gynecology in Department of Obstetrics and Gynecology at Zagazig University Hospital, Egypt; Mena M. Abdalla (MSc) in Department of Obstetrics and Gynecology at Menia Health Insurance Hospital, Egypt.
Rights and permissions
About this article

Cite this article
Elnaggar, E.A., Elwan, Y.A., Ibrahim, S.A. et al. Hormonal Changes After Laparoscopic Ovarian Diathermy in Patients with Polycystic Ovarian Syndrome. J Obstet Gynecol India 66 (Suppl 1), 528–533 (2016). https://doi.org/10.1007/s13224-016-0882-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-016-0882-2