
Abstract
Objectives
There is no conclusive evidence of adverse health effects caused by short-term exposure to coarse particulate matter, so in this case-crossover study we looked for an association between exposure and emergency ambulance dispatches (as a proxy of acute health outcomes).
Methods
We used data on emergency ambulance dispatches in Fukuoka City, Japan between 2005 and 2010. After excluding ambulance dispatches related to external injuries and pregnancy/childbirth, we analyzed data on 176,123 dispatches. Citywide daily mean concentrations of suspended particulate matter (SPM) and fine particulate matter (PM2.5) were calculated from ambient monitoring data, and the differences between concentrations of SPM and PM2.5 were used as an exposure surrogate of coarse particulate matter. Using a conditional logistic regression model, we estimated the ambient temperature and relative humidity adjusted odds ratios (ORs) per 10 μg/m3 increase in coarse particulate matter.
Results
The average daily concentration of coarse particulate matter over the study period was 9.9 μg/m3, representing 33 % of the total concentration of SPM. Elevated concentrations of coarse particulate matter were associated with an increase in respiratory disease-related emergency ambulance dispatches for adults aged 65 years or older (9,716 dispatches, OR for lag0–1 = 1.065, 95 % confidence interval = 1.023–1.109). After additional adjustment for exposure to PM2.5, we observed a statistically non-significant increased risk (OR = 1.035, 0.986–1.086).
Conclusions
We found weak evidence of adverse effects of short-term exposure to coarse particulate matter on human health.
Similar content being viewed by others


Introduction
Accumulating evidence leaves no doubt that particulate matter has adverse effects on human health [1]. The adverse effects of fine particulate matter (PM2.5, i.e., particles that pass through a size-selective inlet with a 50 % cut-off level of 2.5 μm in aerodynamic diameter) have received particular attention in recent years. In 2009, the US Environmental Protection Agency reported a causal relationship between short-term exposure to PM2.5 and mortality and cardiovascular diseases [2]. However, several research questions regarding particulate matter remain unanswered. One concerns the associations between coarse particulate matter and mortality and morbidity. Coarse particulate matter is typically classified as particulate matter measuring between 2.5 and 10 μm (PM10-2.5) in diameter. Unlike fine particles, coarse particles do not reach the alveoli of the lungs [3] but are deposited along the bronchial tubes; they have been associated with pulmonary toxicity [4, 5]. Although exposure to coarse particulate matter is also thought to adversely affect human health, there is no conclusive evidence of causal associations between short-term exposure to coarse particulate matter and mortality and morbidity [2].
Japanese Air Quality Standards [6] apply to suspended particulate matter (SPM that passes through a size-selective inlet with a 100 % cut-off level of 10 μm in aerodynamic diameter) and PM2.5, so PM10 (particles that pass through a size-selective inlet with a 50 % cut-off level of 10 μm in aerodynamic diameter) is not monitored in Japan. In the present study, therefore, we defined the difference between concentrations of SPM and PM2.5 as an exposure surrogate of coarse particulate matter. Our hypothesis was that coarse particulate matter would cause acute health effects. To examine this hypothesis, we conducted time-stratified case-crossover analyses to investigate any association between short-term exposure to coarse particulate matter and emergency ambulance dispatches, which were used as a proxy marker of acute health events. We have previously reported that exposure to PM2.5 was positively associated with ambulance dispatches in Fukuoka City, Japan, where PM2.5 concentrations had measured before Air Quality Standards for PM2.5 were established in 2009 [7]. We used the same dataset in this study.
Materials and methods
Information on emergency ambulance dispatches
The present study was carried out in Fukuoka City, which is on the island of Kyushu in western Japan (130°24′E, 33°35′N); it is the closest part of Japan to the Asian continent. Fukuoka’s population is approximately 1.5 million, and the climate is moderate (average annual temperature: c. 17 °C).
In Japan, local governmental fire defense headquarters provide emergency medical services in accordance with the Local Autonomy Law and Firefighting Acts, with costs covered from tax revenues [8, 9]; ambulance services are thus provided free of charge. We obtained data on all emergency ambulance dispatches covering the entire city of Fukuoka between January 1, 2005 and December 31, 2010 (n = 307,711). After excluding dispatches related to external injuries and pregnancy/childbirth, we were left with data on 176,123 dispatches (57.2 %) for analysis. Records of the initial diagnoses made at the emergency departments where the transported patients were treated were used to code the causes of the dispatches according to the International Classification of Diseases, 10th revision (ICD-10); one medical doctor (TM) masked to exposure information performed all coding. We defined ambulance dispatches related to respiratory diseases (ICD-10: J00-99, 15,857 dispatches) and cardiovascular diseases (ICD-10: I00-99, 31,837 dispatches) as cause specific.
We submitted the study protocol to the Ethical Review Board of the National Institute for Environmental Studies for approval but were told by the Board that approval was not required because the study data did not include individual identifiers.
Environmental data
We obtained data on hourly measurements of SPM, nitrogen dioxide (NO2), photochemical oxidants (Ox) with concentrations nearly equivalent to those of ozone, and sulfur dioxide (SO2) from the National Institute for Environmental Studies’ atmospheric environment database; we obtained data on PM2.5 from Fukuoka City records. The mass concentrations of SPM were measured by β-ray absorption. The 8 ambient pollution monitoring stations representing urban background concentrations in Fukuoka provided data on concentrations of pollutants in the city (Fig. 1), and citywide daily mean concentrations of SPM, NO2, and SO2 and daily maximum 8-h mean concentrations of Ox were calculated by averaging the measurements made by the 8 monitoring stations. In one of these stations, PM2.5 was measured by the tapered element oscillating microbalance method.

Location of monitoring stations and meteorological observatory in Fukuoka City
In the present study, we calculated daily mean concentrations of coarse particulate matter by subtracting daily mean concentrations of PM2.5 from those of SPM. Under Japanese Air Quality Standards [6], SPM is defined as airborne particles with a 100 % cut-off point of 10 μm in aerodynamic diameter. Overseas, PM10 and PM2.5 are usually defined as particles with a 50 % cut-off point of 10 and 2.5 μm, respectively, in aerodynamic diameter. Although the SPM definition does not specify the size of particles collected with a 50 % cut-off point, measurements by the 8 stations in Fukuoka showed a 50 % cut-off point of approximately 7 μm. Therefore, we deduced that SPM concentrations correspond more or less to PM7 concentrations and defined SPM as particles with a 50 % cut-off level of 7 μm in aerodynamic diameter. Thus, coarse particulate matter as defined in this study was taken as PM7-2.5, in the same way as PM10-2.5 was calculated by subtracting PM2.5 from PM10. In Fukuoka, coarse particles consisted mainly of natural particles such as sea-salt and soil particles [10]. During the study period of 2,191 days, SPM measurements were available on all days, and PM2.5 measurements on 2,162 days. On 8 days, there were negative concentrations of coarse particulate matter, so these were excluded, leaving 2,154 days of coarse particulate matter measurements for our analyses.
Meteorological data collected by the Fukuoka District Meteorological Observatory were obtained from the Japan Meteorological Agency: hourly measurements were used to calculate daily mean ambient temperatures and relative humidity. Data on weekly influenza incidence were obtained from the Japan National Institute of Infectious Diseases. Influenza epidemic weeks were defined as those when the weekly number of influenza cases was above the 90th percentile of distribution during the study period [11], and influenza epidemics were used as a dichotomized variable.
Statistical analyses
To assess the association between short-term exposure to coarse particulate matter and emergency ambulance dispatches, we used a time-stratified case-crossover approach. We defined case periods as the days of ambulance dispatches and selected control periods (3–4 per case) on corresponding days of the week within the same calendar month of the same year. For instance, if an outcome occurred on August 14, 2008, we assigned August 7, 21, and 28, 2008 as the 3 control days. With this approach, we were able to adjust for time-invariant characteristics such as age and sex, and time-dependent confounding within strata time by methods [12].
Conditional logistic regression models were used to examine the association between coarse particulate matter and emergency ambulance dispatches. Then, to examine lag pattern of coarse particulate matter and control for confounding by it, we applied a lag-stratified distributed lag model [13] and included the average concentrations of coarse particulate matter during the case day (lag0) to 1 day preceding it (lag1) (lag0–1), during lag2–lag3 (lag2–3), and during lag4–lag6 (lag4–6) [14]. Odds ratios (ORs) for a 10 μg/m3 increase in coarse particulate matter concentrations with 95 % confidence intervals (CIs) were calculated after adjustment for the mean ambient temperature (a natural spline with 4 degrees of freedom) and relative humidity from the case day (lag0) to 3 days before (lag3). We performed stratified analyses by age strata (0–19 years, 20–64 years, and 65 years or older), and using likelihood ratio tests to check whether the effects of coarse particulate matter concentrations on ambulance dispatches were modified by age strata. In addition, we conducted several sensitivity analyses. First, to eliminate the possibility of bias in control selection, we excluded dispatches occurring on national holidays. Second, we excluded dispatches occurring on “Asian dust” days (lag0–3) (Asian dust is mineral dust blown from deserts in China and Mongolia to western Pacific regions [15]). Because exposure to Asian dust is reportedly associated with emergency ambulance dispatches [16], it was important to look for associations between coarse particulate matter concentrations and ambulance dispatches after excluding days of extra-high exposure to this natural coarse particulate matter. Third, we additionally included influenza epidemics in the model. Finally, to evaluate the independent effects of coarse particulate matter, we constructed two-pollutant models adjusted for co-pollutants, namely PM2.5, NO2, Ox, and SO2. Although we took into consideration the effects of season (spring, summer, autumn, and winter) in terms of the association between coarse particulate matter and ambulance dispatches, statistical evidence of effect modification by season was not observed (p for effect modification = 0.31).
Statistical analyses were conducted with Stata11 (Stata Corporation, College Station, TX, USA). All p values are two-sided with significance levels set at p < 0.05.
Results
Of the 176,123 emergency ambulance dispatches, 16,415 (9.3 %) were for the 0- to 19-year-old age group, 79,734 (45.3 %) for the 20- to 64-year-old age group, and 79,974 (45.4 %) for the 65-year or older age group; 86,127 (48.9 %) of the dispatches were for men. Descriptive statistics of exposure data are shown in Table 1. The average daily concentration of coarse particulate matter over the study period was 9.9 μg/m3, representing 33 % of the total concentrations of SPM. Coarse particulate matter concentration correlated moderately with that of PM2.5 (Pearson’s correlation coefficient = 0.49), but not with concentrations of the other pollutants (correlation coefficients = 0.02 for NO2, 0.02 for Ox, and 0.18 for SO2).
We examined the association between exposure and coarse particulate matter and emergency ambulance dispatches (Table 2). All-cause ambulance dispatches were not associated with coarse particulate matter (OR for lag0–1 = 1.006 per 10 μg/m3 increase in coarse particulate matter, 95 % CI = 0.996–1.016). Although a statistically significant association was found in the 65-year or older age group (OR for lag0–1 = 1.020, 95 % CI = 1.005–1.035), there was no evidence of effect modification by age strata (p = 0.65). However, coarse particulate matter was clearly associated with an elevated risk of respiratory disease-related ambulance dispatches for those aged 65 years or older (OR for lag0–1 = 1.065, 95 % CI = 1.023–1.109), and effect modification of exposure to coarse particulate matter across age strata was demonstrated (p = 0.02). Null association was observed for cardiovascular-related ambulance dispatches.
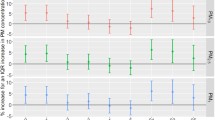
We attempted to confirm the robustness of the positive association we observed with regard to respiratory disease-related ambulance dispatches (Fig. 2). When dispatches occurring on national holidays were excluded (OR for lag0–1 per 10 μg/m3 increase in coarse particulate matter = 1.075, 95 % CI = 1.031–1.122) and additional adjustments were made for influenza epidemics (OR = 1.067, 95 % CI = 1.025–1.111), the results did not change substantially. Although the OR point estimate was slightly higher when ambulance dispatches on Asian dust days were excluded (OR = 1.111, 95 % CI = 1.039–1.189), no significant difference in point estimates on days with or without Asian dust was observed (p for effect modification = 0.31). In the two-pollutant model, our finding was robust after adjustment for NO2, Ox, and SO2; however, the observed effects of coarse particulate matter concentration were not significant after adjustment for PM2.5 (OR per 10 μg/m3 increase = 1.035, 95 % CI = 0.986–1.086) [OR per interquartile range increase (6.3 μg/m3) = 1.022, 95 % CI = 0.991–1.054]. In this case, we found a significantly increased risk for exposure to PM2.5 [OR per interquartile range increase (13.3 μg/m3) for lag0–1 = 1.050, 95 % CI = 1.008–1.094].

Sensitivity analyses of the association between coarse particulate matter (lag0–1) and emergency ambulance dispatches due to respiratory diseases (n = 9,716) in older adults (≥65 years or older). Error bars indicate 95 % confidence intervals
Discussion
On the basis of our previous work [7], we are confident that ambulance dispatches are an adequate indicator of acute health effects of particulate matter exposure. An advantage of using data on emergency ambulance dispatches is that any selection bias was negligible, because we obtained information on all ambulance dispatches in Fukuoka City and covered the whole target population. In the present study, we found that elevated concentrations of coarse particulate matter were associated with an increase in respiratory disease-related emergency ambulance dispatches for adults aged 65 years or older. After adjustment for exposure to PM2.5, however, the OR point estimate was attenuated and the statistical evidence weakened. Exposure to coarse particulate matter was not associated with cardiovascular-related ambulance dispatches.
Although we conclude that short-term exposure to coarse particulate matter might have adverse effects on human health, two possible methodological shortcomings should be noted. First, instead of directly measuring concentrations of coarse particulate matter, we estimated them from the differences between SPM and PM2.5 concentrations. Daily mean concentrations of SPM were calculated by averaging the measurements made by the 8 monitoring stations, whereas those of PM2.5 were estimated from the measurements at one monitoring station. Thus, the estimated concentrations might have been subject to measurement errors. Second, our cause-specific categorizations of ambulance dispatches were based on initial diagnoses made by emergency physicians, and the final diagnoses were probably different in some cases. However, such exposure and outcome misclassifications are generally non-differential, so they are likely to lead to null associations. Despite these possible shortcomings, increasing concentrations of coarse particulate matter resulted in a statistically significant increase in the risk of respiratory disease-related ambulance dispatches for older Japanese adults.
To the best of our knowledge, the present study is the first to investigate the acute health effects of coarse particulate matter (i.e., the difference between SPM and PM2.5) in Japan. We found no evidence of an association between exposure and PM10-2.5 and emergency ambulance dispatches. It is difficult to discuss epidemiological consistency with the past literature, but one study in 35 California counties reported that a 10 µg/m3 increase in PM10-2.5 concentrations for lag1 was associated with a 0.7 % (95 % CI = 0.3–1.1) increase in respiratory emergency room visits from 2005 to 2008 [17]. Another study in Helsinki also reported a positive association between exposure and PM10-2.5 and asthma and chronic obstructive pulmonary disease emergency room visits from 1998 to 2004 (percent change per 7.2 µg/m3 increase for lag0 = 2.70 (95 % CI = 0.21–5.26) for adults (15–64 years) and 2.45 (0.18–4.76) for older adults (≥65 years) [18]. Earlier findings from mechanism studies have demonstrated pulmonary effects of PM10-2.5. Exposure of cells to coarse particles led to increased levels of inflammatory biomarkers such as tumor necrosis factor alpha and interleukin-6 [19, 20]. In rats and mice, exposure to coarse particles contributed to increased pulmonary inflammation [21, 22]. In addition, an increase in inflammatory cells in sputum and bronchoalveolar lavage fluid was observed in healthy young volunteers exposed to coarse particles [4, 5]. Taken as a whole, our results are supported by both epidemiological and experimental evidence.
In the present study, we found a clear association between coarse particulate matter concentrations and respiratory effects only in older adults (aged ≥ 65 years), whereas other studies using PM10-2.5 have also found associations in other age strata. A positive association with respiratory-related emergency visits was observed in children under 15 years of age who lived in Santiago, Chile [23], and associations with asthma and chronic obstructive pulmonary disease emergency room visits were found not only among adults aged 65 years or older but also among those aged 15–64 years old in Helsinki, Finland [18]. Adverse health effects of particulate matter on older adults are not surprising, because recent meta-analysis shows that older populations are more vulnerable to particulate matter than younger populations [24]. In our model including PM2.5, exposure to coarse particulate matter was not statistically significantly associated with respiratory disease-related ambulance dispatches; however, the OR point estimate was still above unity, and there was an overlap between 95 % CI with and without adjustment for PM2.5. Therefore, the non-significance might have resulted from a lack of statistical power due to the relatively small number of cases in the stratified analysis, and we do not think that our finding after adjustment for PM2.5 denies an independent association between coarse particulate matter concentrations and ambulance dispatches. Because the point estimate (interquartile range increase) for the association of coarse particulate matter with ambulance dispatches was slightly lower than that for the association of PM2.5, it seemed likely that the health effects of coarse particulate matter were relatively smaller than those of PM2.5.
Although we observed little effect of coarse particulate matter (the difference between concentrations of SPM and PM2.5) on cardiovascular disease-related emergency ambulance dispatches, several earlier studies in Western countries found the associations between coarse particulate matter defined as PM10-2.5 and mortality and morbidity, including hospital admissions for cardiovascular disease [25]. One possible explanation for the null association in this study is that the breakdown of cardiovascular diseases in Japan is different from that in Western countries. In Japan, the incidence of stroke is much higher than that of coronary heart disease [26]. Therefore, the association between particulate matter and cardiovascular diseases in Japan may also differ from that in Western countries, where coronary heart disease is the most common cardiovascular complaint. It should also be noted that our results lack generalizability, because our study was restricted to one city. The acute cardiovascular effects of coarse particulate matter exposure in Japan require further study.
In conclusion, our findings indicate that short-term exposure to coarse particulate matter (estimated by subtracting concentrations of PM2.5 from those of SPM) might have acute health effects. Japan’s current Air Quality Standards include both SPM and PM2.5 [6], so further epidemiological studies are required to determine whether it is appropriate to regulate SPM and PM2.5 separately.
References
Rückerl R, Schneider A, Breitner S, Cyrys J, Peters A. Health effects of particulate air pollution: a review of epidemiological evidence. Inhal Toxicol. 2011;23:555–92.
US Environmental Protection Agency. Integrated science assessment for particulate matter. Research Triangle Park, NC 2009.
Lippmann M, Chen LC. Health effects of concentrated ambient air particulate matter (CAPs) and its components. Crit Rev Toxicol. 2009;39:865–913.
Alexis NE, Lay JC, Zeman K, Bennett WE, Peden DB, Soukup JM, et al. Biological material on inhaled coarse fraction particulate matter activates airway phagocytes in vivo in healthy volunteers. J Allergy Clin Immunol. 2006;117:1396–403.
Graff DW, Cascio WE, Rappold A, Zhou H, Huang YC, Devlin RB. Exposure to concentrated coarse air pollution particles causes mild cardiopulmonary effects in healthy young adults. Environ Health Perspect. 2009;117:1089–94.
Japanese Ministry of the Environment (2009) Environmental quality standards in Japan –air quality. http://www.env.go.jp/en/air/aq/aq.html. Accessed 14 Nov 2014.
Michikawa T, Ueda K, Takeuchi A, Kinoshita M, Hayashi H, Ichinose T, et al. Impact of short-term exposure to fine particulate matter on emergency ambulance dispatches in Japan. J Epidemiol Community Health. doi:10.1136/jech-2014-203961 (Epub on ahead print).
Tanigawa K, Tanaka K. Emergency medical service systems in Japan: past, present, and future. Resuscitation. 2006;69:365–70.
Hagihara A, Hasegawa M, Hinohara Y, Abe T, Motoi M. The aging population and future demand for emergency ambulances in Japan. Intern Emerg Med. 2013;8:431–7.
Watanabe M, Kobe K, Ohe M, Shinozuka M, K Takahra, T Furukawa. The variation and characteristics of suspended particulate matter in Fukuoka City (part2). Fukuokashihokankenhou. 1997;22:128–33 (Article in Japanese).
Ng CF, Ueda K, Takeuchi A, Nitta H, Konishi S, Bagrowicz R, et al. Sociogeographic variation in the effects of heat and cold on daily mortality in Japan. J Epidemiol. 2014;24:15–24.
Janes H, Sheppard L, Lumley T. Case-crossover analyses of air pollution exposure data: referent selection strategies and their implications for bias. Epidemiology. 2005;16:717–26.
Armstrong B. Models for the relationship between ambient temperature and daily mortality. Epidemiology. 2006;17:624–31.
Ueda K, Nitta H, Odajima H. The effects of weather, air pollutants, and Asian dust on hospitalization for asthma in Fukuoka. Environ Health Prev Med. 2010;15:350–7.
Sugimoto N, Uno I, Nishikawa M, Shimiza A, Matsui I, Dong X, et al. Record heavy Asian dust in Beijing in 2002: Observations and model analysis of recent events. Geophys Res Lett. 2003;30:1640.
Ueda K, Shimizu A, Nitta H, Inoue K. Long-range transported Asian Dust and emergency ambulance dispatches. Inhal Toxicol. 2012;24:858–67.
Malig BJ, Green S, Basu R, Broadwin R. Coarse particles and respiratory emergency department visits in California. Am J Epidemiol. 2013;178:58–69.
Halonen JI, Lanki T, Yli-Tuomi T, Tiittanen P, Kulmala M, Pekkanen J. Urban air pollution, and asthma and COPD hospital emergency room visits. Thorax. 2008;63:635–41.
Pozzi R, De Berardis B, Paoletti L, Guastadisegni C. Inflammatory mediators induced by coarse (PM2.5–10) and fine (PM2.5) urban air particles in RAW 264.7 cells. Toxicology. 2003;183:243–54.
Volckens J, Dailey L, Walters G, Devlin RB. Direct particle-to-cell deposition of coarse ambient particulate matter increases the production of inflammatory mediators from cultured human airway epithelial cells. Environ Sci Technol. 2009;43:4595–9.
Gerlofs-Nijland ME, Dormans JA, Bloemen HJ, Leseman DL, John A, Boere F, et al. Toxicity of coarse and fine particulate matter from sites with contrasting traffic profiles. Inhal Toxicol. 2007;19:1055–69.
Tong H, Cheng WY, Samet JM, Gilmour MI, Devlin RB. Differential cardiopulmonary effects of size-fractionated ambient particulate matter in mice. Cardiovasc Toxicol. 2010;10:259–67.
Ilabaca M, Olaeta I, Campos E, Villaire J, Tellez-Rojo MM, Romieu I. Association between levels of fine particulate and emergency visits for pneumonia and other respiratory illnesses among children in Santiago, Chile. J Air Waste Manag Assoc. 1999;49:154–63.
Bell ML, Zanobetti A, Dominici F. Evidence on vulnerability and susceptibility to health risks associated with short-term exposure to particulate matter: a systematic review and meta-analysis. Am J Epidemiol. 2013;178:865–76.
Brunekreef B, Forsberg B. Epidemiological evidence of effects of coarse airborne particles on health. Eur Respir J. 2005;26:309–18.
Ueshima H, Sekikawa A, Miura K, Turin TC, Takashima N, Kita Y, et al. Cardiovascular disease and risk factors in Asia: a selected review. Circulation. 2008;118:2702–9.
Acknowledgments
We appreciate the help Mr. Hiromi Hayashi (Environmental Bureau of Fukuoka City, Fukuoka, Japan) gave us in acquiring data. We would also like to thank Ms. Noriko Shidai (National Institute for Environmental Studies, Tsukuba, Japan) for her assistance with our work. This study was supported by a Grant-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology, Japan (25241015).
Conflict of interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Michikawa, T., Ueda, K., Takeuchi, A. et al. Coarse particulate matter and emergency ambulance dispatches in Fukuoka, Japan: a time-stratified case-crossover study. Environ Health Prev Med 20, 130–136 (2015). https://doi.org/10.1007/s12199-014-0439-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12199-014-0439-x