
Abstract
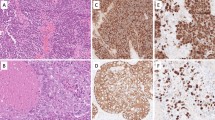
Primary sinonasal tract carcinoma ex-pleomorphic adenoma (CEPA) is very uncommon, with adenoid cystic carcinoma (ACC) CEPA exceptional. These tumors are often misclassified. This is a retrospective study. Nine cases of ACC CEPA included 7 females and 2 males, aged 39–64 years (mean, 51.1 years). Patients presented most frequently with obstructive symptoms (n = 5), epistaxis (n = 3), nerve changes or pain (n = 3), present for a mean of 25 months (men: 9.5 versus women: 29.4 months; p = 0.264). The tumors involved the nasal cavity alone (n = 5), nasopharynx (n = 2), or a combination of locations (n = 2) with a mean size of 2.9 cm (females: 3.3; males: 1.7; p = 0.064). Most patients presented at a low clinical stage (n = 7, stage I), with one patient each in stage II and IV, respectively. Histologically, the tumors showed foci of PA associated with areas of ACC. Tumors showed invasion (lymph-vascular: n = 4; perineural: n = 6; bone: n = 6). The neoplastic cells were arranged in tubules, cribriform and solid patterns, with peg-shaped cells arranged around reduplicated basement membrane and glycosaminoglycan material. Mitoses ranged from 0 to 33, with a mean of 8.7 mitoses/10 HPFs. Necrosis (n = 2) and atypical mitotic figures (n = 1) were seen infrequently. Immunohistochemical studies showed positive reactions for cytokeratin, CK5/6, p63, CK7, EMA, SMA, calponin, S100 protein and CD117, several highlighting luminal versus basal cells components. GFAP, CK20 and MSA were non-reactive. p53 and Ki-67 were reactive to a variable degree. Surgery (n = 8), accompanied by radiation therapy (n = 5) was generally employed. Five patients developed a recurrence, all of whom died with disease (mean, 8.4 years), while 4 patients are either alive (n = 2) or had died (n = 2) without evidence of disease (mean, 15.9 years). In summary, ACC CEPA probably arises from the minor mucoserous glands of the upper aerodigestive tract, usually presenting in patients in middle age with obstructive symptoms in a nasal cavity based tumor. Most patients present with low stage disease (stage I and II), although invasive growth is common. Recurrences develop in about a 55 % of patients, who experience a shorter survival (mean, 8.4 years) than patients without recurrences (mean, 15.9 years). The following parameters, when present, suggest an increased incidence of recurrence or dying with disease: bone invasion, lymph-vascular invasion, and perineural invasion.







Similar content being viewed by others


References
Eveson JW. Salivary gland-type carcinomas. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics: head and neck tumours. Lyon: IARC Press; 2005. p. 24–5.
Franchi A, Santucci M, Wenig BM. Adenocarcinoma. In: Barnes EL, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics head and neck tumours. Lyon: IARC Press; 2005. p. 20–3.
Kleinsasser O, Schroeder HG. Adenocarcinomas of the inner nose after exposure to wood dust. Morphological findings and relationships between histopathology and clinical behavior in 79 cases. Arch Otorhinolaryngol. 1988;245:1–15.
Barnes L. Intestinal-type adenocarcinoma of the nasal cavity and paranasal sinuses. Am J Surg Pathol. 1986;10:192–202.
Gnepp DR, Heffner DK. Mucosal origin of sinonasal tract adenomatous neoplasms. Mod Pathol. 1989;2:365–71.
Cimino-Mathews A, Lin BM, Chang SS, Boahene KD, Bishop JA. Carcinoma ex pleomorphic adenoma of the nasal cavity. Head Neck Pathol. 2011;5:405–9.
Freeman SR, Sloan P, de Carpentier J. Carcinoma ex-pleomorphic adenoma of the nasal septum with adenoid cystic and squamous carcinomatous differentiation. Rhinology. 2003;41:118–21.
Shukla NK, Hazarika S, Deo S, Kar M, Kumar S, Samaiya A, et al. Salivary gland tumours: profile and management at a tertiary cancer centre. J Indian Med Assoc. 2011;109:381–5.
Nordkvist A, Roijer E, Bang G, Gustafsson H, Behrendt M, Ryd W, et al. Expression and mutation patterns of p53 in benign and malignant salivary gland tumors. Int J Oncol. 2000;16:477–83.
Saleh ER, Franca CM, Marques MM. Neural adhesion molecule (N-CAM) in pleomorphic adenoma and carcinoma ex-pleomorphic adenoma. J Oral Pathol Med. 2003;32:562–7.
Perez DE, Pires FR, Almeida OP, Kowalski LP. Epithelial lacrimal gland tumors: a clinicopathological study of 18 cases. Otolaryngol Head Neck Surg. 2006;134:321–5.
Katori H, Nozawa A, Tsukuda M. Increased expression of cyclooxygenase-2 and Ki-67 are associated with malignant transformation of pleomorphic adenoma. Auris Nasus Larynx. 2007;34:79–84.
Ding CS, Yap WM, Teo CH, Giron D, Chuah KL. Tracheal carcinoma ex pleomorphic adenoma: a rare tumour with potential problems in diagnosis. Histopathology. 2007;51:868–71.
Ide F, Mishima K, Yamada H, Saito I. Adenoid cystic carcinoma ex pleomorphic adenoma of the parotid gland. Head Neck Pathol. 2009;3:159–62.
Kuo YL, Tu TY, Chang CF, Li WY, Chang SY, Shiao AS, et al. Extra-major salivary gland pleomorphic adenoma of the head and neck: a 10-year experience and review of the literature. Eur Arch Otorhinolaryngol. 2011;268:1035–40.
Farman AG, George DI Jr, Clear RM. Computerized tomography of combined carcinomas arising in pleomorphic adenoma. Oral Surg Oral Med Oral Pathol. 1985;59:96–101.
Schramm VL Jr, Imola MJ. Management of nasopharyngeal salivary gland malignancy. Laryngoscope. 2001;111:1533–44.
Chimona TS, Koutsopoulos AV, Malliotakis P, Nikolidakis A, Skoulakis C, Bizakis JG. Malignant mixed tumor of the nasal cavity. Auris Nasus Larynx. 2006;33:63–6.
AJCC Cancer Staging Manual, 7th ed. New York: Springer; 2009.
Lewis JE, Olsen KD, Sebo TJ. Carcinoma ex pleomorphic adenoma: pathologic analysis of 73 cases. Hum Pathol. 2001;32:596–604.
Gnepp DR. Malignant mixed tumors of the salivary glands: a review. Pathol Annu. 1993;28(Pt 1):279–328.
Wenig BL, Sciubba JJ, Cohen A, Abramson AL. Pleomorphic adenoma of the nasal septum. Otolaryngol Head Neck Surg. 1985;93:432–6.
Cho KJ, el-Naggar AK, Mahanupab P, Luna MA, Batsakis JG. Carcinoma ex-pleomorphic adenoma of the nasal cavity: a report of two cases. J Laryngol Otol. 1995;109:677–9.
Carinci F, Curioni C, Padula E, Calearo C. Cancer of the nasal cavity and paranasal sinuses: a new staging system. Int J Oral Maxillofac Surg. 1996;25:34–9.
Wolfish EB, Nelson BL, Thompson LD. Sinonasal tract mucoepidermoid carcinoma: a clinicopathologic and immunophenotypic study of 19 cases combined with a comprehensive review of the literature. Head Neck Pathol. 2012;6(2):191–207.
Acknowledgments
The authors thank Ms. Hannah Herrera for her research assistance. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of Southern California Permanente Medical Group.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Toluie, S., Thompson, L.D.R. Sinonasal Tract Adenoid Cystic Carcinoma Ex-Pleomorphic Adenoma: A Clinicopathologic and Immunophenotypic Study of 9 Cases Combined with a Comprehensive Review of the Literature. Head and Neck Pathol 6, 409–421 (2012). https://doi.org/10.1007/s12105-012-0381-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12105-012-0381-4