
Abstract
The purpose of this study was to evaluate the efficacy of transoral or transnasal endoscopic-guided adenoidectomy compared with endoscopic nasopharyngeal inspection at the end of curettage adenoidectomy. A prospective case series of patients who had adenoidectomy. A total of 27 girls and 34 boys (age range 2.5–18 years) in whom adenoidectomy with or without tonsillectomy procedure was planned were included in the study. The cases were divided into three groups. Group 1 Transoral endoscopic-guided adenoidectomy performed patients. Group 2 Transnasal endoscopic-guided adenoidectomy performed patients. Group 3 Transnasal endoscopic nasopharyngeal exploration performed at the end of the conventional curettage adenoidectomy. The study was completed on 61 children. Mean age and sex frequency were not significant different between the groups. Mean operative time were 11.6 ± 2.9, 15.6 ± 4.4 and 9.7 ± 2 min, respectively (p > 0.05). On the other hand, significant differences were observed in operative time between group 1 and group 2 (p < 0.05), and between group 2 and group 3 (p < 0.05). Transnasal endoscopic examination at the end of curettage adenoidectomy is an appropriate method to assess the residual adenoid tissue after conventional curettage adenoidectomy. Also, operative time of this method is shorter than transoral or transnasal endoscopic-guided adenoidectomy. We recommend transnasal endoscopic inspection in all patients after conventional curettage adenoidectomy.
Similar content being viewed by others

Introduction
Adenoidal hypertrophy is a common cause of airway obstruction in children and can cause symptoms such as nasal discharge, mouth breathing, nasal obstruction, snoring, sleep apnea, hyponasal speech, orofacial growth disturbance, otitis media with effusion, recurrent otitis media and rhinosinusitis [1–3]. Adenoidectomy is often indicated in patients with these complaints. Adenoidectomy with or without tonsillectomy and/or ventilation tube insertion is one of the most common surgical procedure in the pediatric population. Several adenoidectomy techniques have been described in the literature. The most common and classical adenoidectomy method is blindly transoral removal of the adenoid tissue with an adenoid curette or adenotome [1, 3, 4]. After conventional curettage adenoidectomy, residual adenoid tissue may remain. Therefore, alternative surgical methods have been described [3, 4].
In this study, transoral or transnasal endoscopic-guided adenoidectomy was compared with endoscopic nasopharyngeal inspection at the end of curettage adenoidectomy.
Materials and Methods
We prospectively performed this clinical study in patients who had undergone adenoidectomy with or without tonsillectomy in the Department of Otorhinolaryngology of Duzce University Medical Faculty from November 2012 till July 2013. This study was approved by the ethics committee of the Abant İzzet Baysal University (No: 2012/186). Written informed consents were obtained from the parents of the patients. The patients were all candidates for elective adenoidectomy and adenotonsillectomy. Patients’ age, sex, indication for surgery, performed surgical procedure, operative time, complications and whether residual adenoid tissue was recorded. Obstructive adenoid tissue was defined when the adenoidal tissues obstruct more than 50 % of the choanal opening in our operated patients. In this study, we evaluated the intraoperative effectiveness of 3 different operation technique not long term results of operations. The operations were performed by the same surgeon with the same two residents. Patients with previous history of adenoidectomy, cases with craniofacial anomalies such as Down’s syndrome and cleft palate, neurological diseases and cardiovascular diseases were excluded from the study. Patients who had recurrent adenoidectomy were also excluded.
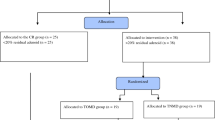
Patients were divided into three groups according to the applied adenoidectomy technique and randomized according to outpatient admission number.
- Group 1:
-
Transoral endoscopic-guided with a 45°, 4 mm rigid fiber-optic telescope (Storz, Germany) adenoidectomy with adenoid curette via transoral way
- Group 2:
-
Transnasal endoscopic-guided with a 30°, 2.7 mm rigid fiber-optic telescope (Storz, Germany), adenoidectomy with adenoid curette via transoral way
- Group 3:
-
Transnasal endoscopic nasopharyngeal exploration with a 30°, 2.7 mm rigid fiber-optic telescope (Storz, Germany) performed at the end of the conventional curettage adenoidectomy
All cases were operated under general anesthesia with orotracheal intubation. After the patient was placed in the standard Rose position in preparation for operation, a mouth gag was inserted and a black feeding catheter was inserted into one of the right or left nares and out of the mouth and then clamped to elevate the soft palate. Transoral or transnasal endoscopic-guided adenoidectomy with adenoid curette was performed in group 1 and 2, respectively. Conventional curettage adenoidectomy was performed in group 3. A nasopharyngeal temporary packing was placed for hemostasis and removed after waiting for approximately 3 min. After removal of the package, we performed nasal irrigations and aspirations to remove blood clots and mucous secretions. Then the nasopharynx was examined with endoscope inserted through the nose for the presence of possible residual tissue in group 3. In patients with residual adenoid tissue, complete adenoidectomy was performed with adenoid currate or forceps under transnasal-guided endoscopic vision. A tonsillectomy was then performed after removal of the nasopharyngeal package and operative time was recorded.
The operative time was recorded. We compared the operative time between the 3 groups. The operative time was defined as the time between the insertion of mouth gag and removal of nasopharyngeal packages in group 1 and 2. In group 3, the operative time was defined as the time between the insertion of mouth gag and removal of nasopharyngeal package or residual adenoid tissue. Antibiotics and analgesics were given for 1 week postoperatively.
Data analysis and all statistical tests were performed using SPSS forWindows (version 16; SPSS Inc., Chicago, IL). Results were given as mean ± standard deviation or percentage. Operative times were compared for the groups using Chi square analysis. A result of p < 0.05 was accepted as significant.
Results
The study was completed on 61 children. Of these patients, 27 were male (44.3 %) and 34 were female (55.7 %). Their ages ranged between 2.5 and 18 years (with a mean of 7.4 ± 3.3). Of the 20 children who underwent transoral endoscopic-guided adenoidectomy (group 1), 8 were male and 12 were female, with ages ranging from 4 to 15 years (mean age, 7.6 ± 2.6 years). Of the 16 children who underwent transnasal endoscopic-guided adenoidectomy (group 2), 9 were male and 7 were female, with ages ranging from 2.5 to 16 years (mean age, 8 ± 4.1 years). Of the 25 children who underwent conventional curettage adenoidectomy (group 3), 17 were male and 8 were female, with ages ranging from 2.5 to 18 years (mean age, 6.8 ± 3.3 years). Mean age and sex frequency were not significant different between the groups. While only adenoidectomy was performed in 21 (34.4 %) patients, adenoidectomy with tonsillectomy was performed in 40 (65.6 %) patients.
The mean operative time for group 1 was 11.6 ± 2.9 min (range, 8–20 min). Group 2 required a mean operative time of 15.6 ± 4.4 min (range, 8–22 min). A mean operative time of 9.7 ± 2 min (range, 6–13 min) was recorded for group 3. There were no statistically significant differences in operative time between group 1 and group 3 (p = 0.091). On the other hand, statistically significant differences were observed in operative time between group 1 and group 2 (p = 0.001), and between group 2 and group 3 (p < 0.001).
Residual adenoid tissues were detected and complete adenoidectomy performed with adenoid curette in 8 (32 %) cases in group 3. Because endoscopic-guided adenoidectomy was performed in group 2 and 3, no residual adenoid tissue was present in these groups. All the procedures were done without any intraoperative or postoperative complications.
Discussion
Adenoidectomy achieves recovery the quality of life and health status of the children. The main goal of this operation is to leave without any macroscopic remnant adenoid tissue. Various adenoidectomy techniques, such as transoral removal of the adenoid tissue with an adenoid curette or adenotome blindly or guided by an indirect mirror, transnasally or transorally adenoidectomy under endoscopic visualization, power-assisted adenoidectomy, suction electrical coagulator adenoidectomy and adenoidectomy with microdebrider have been described in the literature [5–10].
The safety and efficacy of power-assisted endoscopic adenoidectomy were compared with the conventional curettage adenoidectomy in several investigations [5–9]. While blindly transoral removal of the adenoid tissue with an adenoid curette is the most common procedure, a simple and quick adenoidectomy method can remain residual adenoid tissue and can damage important structures such as nasopharyngeal mucosa, torus tubarius and choana [11, 12]. In this method, surgeons frequently check the nasopharynx by digital palpation or sometimes with a laryngeal mirror. Significant residual adenoid tissue rates were reported after curettage adenoidectomy, especially in the torus tubarius and the pharyngeal roof near choanal openings. Abdel-Aziz [3] found that residual adenoid tissue could remain in 20.5 % of the patients following conventional adenoidectomy. He compared the efficacy of postoperative endoscopic examination after conventional adenoidectomy. Recurrence rate was significantly lower in these patients after 2 years of follow up regarding their counterparts who had not undergone endoscopic examination. Elnashar et al. [11] reported 95.45 % of the cases had residual adenoid tissue after conventional curettage adenoidectomy. Patients aged 10 years or more had more residual adenoid tissue after curettage adenoidectomy [11]. They showed that curettage technique is sufficient to remove the adenoids in younger children. On the other hand, they recommended endoscopic-assisted adenoidectomy especially in patients over 10 years of age. Ark et al. [10] found residual adenoid tissue in 79.8 % of patients after blunt curettage and digital palpation. They have evaluated the presence of the residual adenoid tissue with a laryngeal mirror. They concluded that digital palpation is not a reliable method and visualization of the nasopharynx is important for a complete adenoidectomy. El-Badrawy and M. Abdel-Aziz [2] performed transoral endoscopic-guided adenoidectomy using the adenoid curette and forceps similar to our first group of patients. Wan et al. [5] performed nasal endoscopic-guided adenoidectomy using a classic adenoid curette. They suggest this technique as an alternative to conventional adenoidectomy. We treated our second group of patients with this technique. Cannon et al. [1] performed transnasal endoscopic view at the end of the conventional adenoidectomy. They established residual adenoid tissue in their all cases of except for 5.1 % patients and accomplished complementary adenoidectomy under direct visualization with adenoid currates and forceps. For this reason, they suggested direct visualization should be routinely used. Our third group of patients was examined with transnasal endoscopy after conventional adenoidectomy. We have routinely checked nasopharynx with the transnasal endoscope at the end of the conventional curettage adenoidectomy. In our cohort residual adenoid tissue was found in 32 % after curettage adenoidectomy. Some surgeons used a power-assisted adenoidectomy method with or without endoscopic vision. Performing adenoidectomy under the endoscopic view provides direct vision of the operation area, removing adenoidal tissue without removing a residue and decreases the risk of injuring the nasopharynx structures. Koltai et al. [6] compared power-assisted adenoidectomy with conventional transoral adenoidectomy and concluded that it has advantages on conventional technique. However, transnasal or transoral powered-endoscopic methods require expensive equipment, movement of the surgical instruments into the nasopharynx are difficult and the procedure needs prolonged operative time [6, 8, 12, 13]. Also, transnasal endoscopic approaches cause nasal mucosal injuries and bleeding in presence of a septal deviation [10, 11]. Havas and Lowinger detected [14] residual adenoid tissue in 39 % of patients after conventional curettage adenoidectomy. They performed complementary adenoidectomy with transnasal powered-shaver.
Conclusion
Transoral or transnasal endoscopic adenoidectomy has the advantage of direct vision of the nasopharynx during operation. The method avoids injury of important structures and enables complete removal of the adenoidal tissues. However, operative time increases and maneuverability is difficult into the nasopharynx which may need experience and a longer duration of learning curve. The present study showed that transoral or transnasal endoscopic adenoidectomy has no advantage over endoscopic nasopharyngeal examination at the end of conventional curettage. Therefore a simple procedure such as conventional adenoidectomy should not be complicated with the routine use of transoral or transnasal endoscopy. Conventional surgery is reliable and does not carry a risk of trauma of torus tubarius providing that the procedure was undertaken medially. Transnasal endoscopic nasopharyngeal examination at the end of conventional curettage adenoidectomy is effective and appropriate method to assess residual adenoid tissue. Additionally, the operative time was reasonably short. We recommended that transnasal endoscopic examination should be performed to all patients in order to control residual adenoid tissue and buffers in the nasopharynx after conventional curettage adenoidectomy.
References
Cannon CR, Replogle WH, Schenk MP (1999) Endoscopic-assisted adenoidectomy. Otolaryngol Head Neck Surg 121:740–744
El-Badrawy A, Abdel-Aziz M (2009) Transoral endoscopic adenoidectomy. Int. J Otolaryngol 2009(2009):949315. doi:10.1155/2009/949315
Abdel-Aziz M (2012) Endoscopic nasopharyngeal exploration at the end of conventional curettage adenoidectomy. Eur Arch Otorhinolaryngol 269:1037–1040
Yıldırım YS, Apuhan T, Aksoy F, Veyseller B, Ozturan O (2014) Is Transnasal Endoscopic Examination Necessary Before and after adenoidectomy? Indian J Otolaryngol Head Neck Surg. 66:257–260
Wan YM, Wong KC, Ma KH (2005) Endoscopic-guided adenoidectomy using a classic adenoid curette: a simple way to improve adenoidectomy. Hong Kong Med J 11:42–44
Koltai PJ, Kalathia AS, Stanislaw P, Heras HA (1997) Power-assisted adenoidectomy. Arch Otolaryngol Head Neck Surg 123:685–688
Costantini F, Salamanca F, Amaina T, Zibordi F (2008) Videoendoscopic adenoidectomy with microdebrider. Acta Otorhinolaryngol Ital 28:26–29
Stanislaw PJr, Koltai PJ, Feustel PJ (2000) Comparison of power-assisted adenoidectomy vs adenoid curette adenoidectomy. Arch Otolaryngol Head Neck Surg 126:845–849
Wynn R, Rosenfeld RM (2003) Outcomes in suction coagulator adenoidectomy. Arch Otolaryngol Head Neck Surg 129:182–185
Ark N, Kurtaran H, Ugur KS, Yilmaz T, Ozboduroglu AA, Mutlu C (2010) Comparison of adenoidectomy methods: examining with digital palpation versus visualizing the placement of the curette. Int J Pediatr Otorhinolaryngol 74:649–651
Elnashar I, El-Anwar MW, Basha WM, AlShawadfy M (2014) Objective assessment of endoscopy assisted adenoidectomy. Int J Pediatr Otorhinolaryngol. 2014 May 14. pii: S0165–5876(14)00243-2. doi: 10.1016/j.ijporl.2014.04.031. [Epub ahead of print]
Yanagisawa E, Weaver EM (1997) Endoscopic adenoidectomy with the microdebrider. Ear Nose Throat J 76:72–74
Öztürk Ö, Polat Ş (2012) Comparison of transoral power-assisted endoscopic adenoidectomy to curettage adenoidectomy. Adv Ther 29:708–721
Havas T, Lowinger D (2002) Obstructive adenoid tissue: an indication for powered-shaver adenoidectomy. Arch Otolaryngol Head Neck Surg 128:789–791
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yaman, H., Memis, M. & Ilhan, E. Comparison of Transoral/Transnasal Endoscopic-Guided Adenoidectomy with Endoscopic Nasopharyngeal Inspection at the End of Curettage Adenoidectomy. Indian J Otolaryngol Head Neck Surg 67, 124–127 (2015). https://doi.org/10.1007/s12070-014-0775-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-014-0775-6