
Abstract
Background
Stroke is common after aneurysmal subarachnoid hemorrhage (aSAH). Transcranial Doppler ultrasound (TCD) monitoring is often employed to identify vasospasm and allow intervention to avoid infarction. The required duration of monitoring has not been established. We aim to determine if 10 days of TCD monitoring identifies all patients at risk for infarction.
Methods
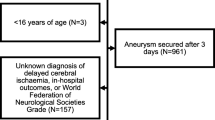
A 3 year retrospective analysis of aSAH patients admitted to a neurovascular center was undertaken. Eligible patients were aged 18–85 years, presenting within 2 days of hemorrhage who had underwent TCD monitoring through post bleed day 10. Patients were assessed to determine if vasospasm onset occurred after 10 days with resulting stroke. Assessment of variables potentially impacting vasospasm onset and infarction were completed.
Results
107 patients met criteria with 51 (48%) demonstrating vasospasm and 31 (29%) developing stroke. Of those suffering stroke, 22 (71%) demonstrated vasospasm while 9 (22%) did not. Two (2%) patients developed vasospasm only after day 10, neither experiencing stroke. Time to vasospasm onset (5.5 ± 2.5 days) was not impacted by common radiologic or clinical scales. Glasgow Coma Scale (GCS), Hunt and Hess Score (H&H), WFNS, ventriculostomy placement, intubation, and intraventricular hemorrhage were associated with likelihood of stroke (P < 0.05). The negative predictive value of TCD for identifying stroke risk was 84% while the sensitivity was 71%.
Conclusions
TCD identification of vasospasm after day 10 is rare. Stroke is more likely to result from poor detection than from brevity of TCD monitoring. Improved or alternative monitoring is needed to effectively identify ischemia and prevent stroke.


Similar content being viewed by others


References
King JT. Epidemiology of aneurysmal subarachnoid hemorrhage. Neuroimaging Clin N Am. 1997;7(4):659–68.
Ferguson S, MacDonald RL. Predictors of cerebral infarction in patients with aneurysmal subarachnoid hemorrhage. Neurosurgery. 2007;60:658–67.
Frontera JA, Claassen J, Schmidt JM, Wartenberg KE, Temes R, Connolly ES Jr, et al. Prediction of symptomatic vasospasm after subarachnoid hemorrhage: the modified fisher scale. Neurosurgery. 2006;59:21–7.
Harrod CG, Bendok BR, Batjer HH. Prediction of cerebral vasospasm in patients presenting with aneurysmal subarachnoid hemorrhage: a review. Neurosurgery. 2005;56:633–54.
Skjoth-Rasmussen J, Schulz M, Kristensen S, Bjerre P. Delayed neurological deficits detected by an ischemic pattern in the extracellular cerebral metabolites in patients with aneurysmal subarachnoid hemorrhage. J Neurosurg. 2004;100:8–15.
Schmidt JM, Wartenberg KE, Fernandez A, Claassen J, Rincon F, Ostapkovich ND, et al. Frequency and clinical impact of asymptomatic cerebral infarction due to vasospasm after subarachnoid hemorrhage. J Neurosurg. 2008;109:1052–9.
Alexandrov AV, Sloan MA, Wong LK, Douville C, Razumovsky QY, Koroshetz WJ, et al. Practice standards for transcranial Doppler ultrasound: part 1—test performance. J Neuroimaging. 2007;17(1):11–8.
Janardhan V, Biondi A, Riina HA, Sanelli PC, Steig PE, Gobin YP. Vasospasm in aneurysmal subarachnoid hemorrhage: diagnosis, prevention, and management. Neuroimag Clin N Am. 2006;16:483–96.
Fisher CM, Kistler JP, Davis JM. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery. 1980;6:1–9.
Drake CG, Hunt WE, Sano K. Report of World Federation of Neurological Surgeons Committee on a universal subarachnoid hemorrhage grading scale. J Neurosurgery. 1988;68:985–6.
Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg. 1968;28(1):14–20.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–4.
Bederson JB, Connolly ES Jr, Batjer HH, Dacey RG, Dion JE, Diringer MN, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 2009;40(3):994–1025.
Ramakrishna R, Stiefel M, Udoteuk J, Spiotta A, Levine JM, Koftke A, et al. Brain oxygen tension and outcome in patients with aneurysmal subarachnoid hemorrhage. J Neurosurg. 2008;109:1075–82.
Vespa PM, O’Phalen K, McArthur D, Miller C, Eliseo M, Hirt D, et al. Pericontusional brain tissue exhibits persistent elevation of lactate/pyruvate ratio independent of cerebral perfusion pressure. Crit Care Med. 2007;35(4):1153–60.
Sarrafzadeh AS, Haux D, Ludemann L, Amthauer H, Plotkin M, Kuchler I, et al. Cerebral ischemia in aneurysmal subarachnoid hemorrhage: a correlative microdialysis-PET study. Stroke. 2004;35(3):638–43.
Hnafy KA, Grobelny B, Fernandez L, Kurtz P, Connolly ES, Mayer SA, et al. Brain interstitial fluid TNF-alpha after subarachnoid hemorrhage. J Neurol Sci. 2010;291:69–73.
McMahon CJ, McDermott P, Horsfall D, Selvarajah JR, King AT, Vail A. The reproducibility of transcranial Doppler middle cerebral artery velocity measurements: implications for clinical practice. Br J Neurosurg. 2007;21(1):21–7.
Carrera E, Schmidt JM, Oddo M, Fernandez L, Claasen J, Seder D, et al. Transcranial Doppler for predicting delayed ischemia after subarachnoid hemorrhage. Neurosurgery. 2009;65:316–24.
Disclosure
The authors report no conflict of interest concerning materials or methods used in this study or the findings specified in this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Miller, C.M., Palestrant, D., Schievink, W.I. et al. Prolonged Transcranial Doppler Monitoring After Aneurysmal Subarachnoid Hemorrhage Fails to Adequately Predict Ischemic Risk. Neurocrit Care 15, 387–392 (2011). https://doi.org/10.1007/s12028-011-9564-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-011-9564-1