
Abstract
A vicious cycle of airway obstruction, infection, and inflammation continues to cause most of the morbidity and mortality in cystic fibrosis (CF). Mutations that result in decreased expression or function of the membrane Cl− channel, cystic fibrosis transmembrane regulator (CFTR), result in a decrease in the volume (and hence the depth) of liquid on the airway surface, impaired ciliary function, and dehydrated glandular secretions. In turn, these abnormalities contribute to a milieu, which promotes chronic infection with a limited but unique spectrum of microorganisms. Defects in CFTR also perturb regulation of several intracellular signaling pathways including signal transducers and activator of transcription, I-κB and nuclear factor-kappa B, and low molecular weight GTPases. Together, these abnormalities result in excessive production of NF-κB dependent cytokines such as interleukin (IL)-1, tumor necrosis factor (TNF), IL-6, and IL-8. There are decreased responses to interferon gamma and transforming growth factor beta leading to decreased production of iNOS and NO. Abnormalities of lipid mediators and decreased secretion of counter/regulatory cytokines have also been reported. Together, these effects combine to create a chronic inflammatory process, which damages and obstructs the airways, and eventually claims the life of the patient.
Similar content being viewed by others


Introduction
Cystic fibrosis (CF) [OMIM 602421] is an autosomal recessive disease caused by mutations in the gene on chromosome 7 encoding a 175-kD glycoprotein, the cystic fibrosis transmembrane conductance regulator (CFTR) [1]. More than 1,500 different mutations have been identified (www.genet.sickkids.on.ca/cftr/), which lead to impaired function and/or reduced plasma membrane expression of CFTR [1]. The most common mutation in patients of Northern European descent is a deletion of three nucleotides resulting in the loss of a single phenylalanine residue at position 508 (ΔF508), which causes misfolding of CFTR. The abnormal molecule is retained in the endoplasmic reticulum and does not reach the plasma membrane. In model membranes, ΔF508 CFTR has impaired Cl− channel function. The ΔF508 mutation typically results in a clinically severe (i.e., classical pancreatic insufficient) form of CF [2, 3]. Other mutations may allow residual CFTR function and can present with milder (i.e., nonclassical and, sometimes, pancreatic sufficient) phenotypes [2, 3]. Some mutations do not result in clinical CF but may cause congenital absence of the vas deferens, leading to sterility [4]. Additionally, several important modifying genes can impact the overall clinical severity of the disease [5, 6].
CFTR functions primarily as a cyclic AMP (cAMP)-regulated chloride channel in the apical membranes of epithelial cells, particularly in exocrine glands, sweat ducts, and the airways, among other tissues [7]. By regulating chloride conductance, CFTR influences the ion and water content of luminal secretions. Additionally, CFTR affects the function of other channels in the epithelium [8–12], most notably the amiloride-sensitive epithelial sodium channel (ENaC), which is a major determinant of salt and water transport in the airways [13]. ENaC is expressed in airway and alveolar epithelium but is normally relatively inactive. When activated, it resorbs Na+ (with chloride and water following) from airway surface liquid (ASL). Recent investigations suggest that ASL is isotonic [14–18], and its volume is regulated by the amount of the NaCl on the epithelial surface. The activity of ENaC in normal airways is downregulated by functional CFTR. In the absence of CFTR function (i.e., cystic fibrosis), ENaC activity increases [9–12, 14–19], thereby increasing salt and water resorption across the epithelium. The combination of increased Na+ resorption through ENaC and decreased Cl− secretion through CFTR decreases the amount of isotonic fluid on the airway surface [17–19]. This decreases the height of the periciliary fluid and impairs ciliary function [14–19]. Additionally, glandular secretions are under-hydrated, and mucous may fail to spread normally on top of the ASL layer [15]. Together these abnormalities cause inspissated mucus to plug the ducts of submucosal glands and small airways, as well as the ducts of exocrine organs (e.g. pancreas and biliary system), ultimately leading to obstruction and loss of organ function. In the ducts of sweat glands, CFTR primarily functions in Cl− resorption, so defects in CFTR cause elevated concentrations of NaCl in sweat [20]. This is the basis for the “sweat test,” which is commonly used in the diagnosis of CF [21]. In the intestine of normal individuals, CFTR can be activated by molecules like cholera toxin, which increase intracellular cAMP levels, and will increase luminal Cl− secretion, causing diarrhea. This observation has led to speculation that resistance to the secretory diarrhea of cholera due to defects in CFTR has selected for the high carrier rate of CF mutations in certain populations [22, 23].
Onset of Lung Inflammation in CF
At birth, the CF lung appears free from inflammation or airway obstruction [24–26]. However, the underlying ion transport defects are present. The cycle of mucus stasis with airway obstruction and impaired clearance of infectious agents becomes important as soon as the baby comes into a non-sterile environment. Typically, within the first several months of life, one can detect a heightened inflammatory state [27, 28] characterized by high concentrations of neutrophils (PMNs) in the airways. The PMN release pro-inflammatory mediators and large amounts of active elastase [29, 30]. This contrasts with normal airways, which contain very few PMNs and no detectable active elastase, as protease inhibitors including alpha-1-antitrypsin are in excess [30]. Vastly elevated numbers of PMNs and active elastase can usually be detected by bronchoalveolar lavage (BAL) within the first year of life, even in the absence of positive bacterial cultures [29–31]. This has led to speculation that the inflammatory process in CF is autonomous and begins with a response to the misfolded CFTR protein within the epithelial cells [32]. However, other studies suggest that inflammation is initiated in response to infection, which, early in the disease, can be transiently eradicated [33–37]. Regardless of the initial source of stimulation, considerable data suggests that the inflammatory response is exaggerated and is not normally terminated, persisting well beyond the eradication of the earliest infections [33, 38]. With modern pancreatic enzyme preparations and nutritional support, it is the persistent airway infection and inflammatory response that claims the lives of the majority of patients [39]. Statistical analyses show that the expected median age for survival of currently living CF patients is about 36 years [40].
Setting the Stage: Role of Obstruction and Infection
In the normal lung, cilia project from the epithelial cells into the ASL and beat in coordinated waves to propel mucus out of the lungs. This mucociliary clearance eliminates particles and pathogens from the lungs and is an important part of the innate host defense. Ciliary function is impaired by the reduced depth of ASL in CF [18]. Additionally, dehydrated mucus plugs may obstruct small airways, creating microenvironments with decreased oxygen tension. The decreased mucociliary clearance and obstructed airways trap bacteria, and unique species are selected by the low oxygen tension. Pseudomonas and other organisms, which can adapt to this environment, may be protected from host defenses by the dense mucus and by extracellular polysaccharides secreted by the bacteria. The resulting chronic bacterial infection then serves as a perpetual stimulus for a relentless inflammatory response. The inflammatory response itself is dysregulated and eventually leads to permanent damage to the airways, destruction of the lungs, and death. This inflammatory response and our current understanding of how it escapes from normal control mechanisms is the subject of this review.
Airway Obstruction
Despite much promising research, we are still unable to correct the underlying defects in ion transport or compensate for them to normalize mucociliary transport in small airways. Thus, major targets of therapy include downstream effects such as airway obstruction. Because poor mucus transport is a pivotal contributor to airway obstruction, physical means of augmenting airway clearance have been a hallmark of CF care for many years. These serve to transmit vibration to the airway walls, thereby loosening the thickened mucus so it can be expectorated. Airway clearance therapies may be combined with aerosolized medications such as bronchodilators, rhDNAse, and/or hypertonic saline. Millions of PMNs in the CF airways undergo necrosis and release their DNA as intact long strands, as opposed to undergoing apoptosis, which would result in cleavage of the DNA into small fragments. Daily inhalation of rhDNAse (Pulmozyme®) leads to demonstrable improvements in airway clearance and reduced loss of lung function as measured by spirometry [41–43]. Recently, much attention has been focused on the use of inhaled hypertonic saline to draw in fluid into the airways, thereby augmenting the amount of ASL and improving airway clearance [44, 45]. Future studies documenting long-term clinical outcomes will help to define its role in improving airway clearance.
Infection
Despite efforts to minimize mucus stasis and airway obstruction, endobronchial infection inevitably occurs. A narrow spectrum of bacteria, some of which express unique adaptations, chronically infects the airways of most patients with CF [46, 47]. The process of selection for this limited spectrum of pathogens is not fully understood. Early on, Staphylococcus aureus and Haemophilus influenzae predominate. These organisms are replaced or accompanied by Gram-negative bacilli in later childhood. Beyond early childhood, most patients become infected with Pseudomonas aeruginosa. Chronic, ineradicable infection with this organism is widely prevalent by adolescence or young adulthood and usually heralds an accelerated rate of decline in lung function. Many patients eventually also become infected with other unusual bacteria such as Stenotrophomonas maltophilia, Alcaligenes xylosoxidans, and/or Burkholderia cepacia complex organisms. Recurrent infections with Mycobacterium avium and fungi are not uncommon, particularly in older patients. In addition to the impaired mucociliary clearance, the eradication of pseudomonas from CF airways is further hampered by this pathogen’s ability to form mucoid microcolonies and biofilms [48, 49]. The dense exopolysaccharide matrix produced by organisms growing as biofilms or organized colonies within the lungs serves to protect the bacteria from phagocytes, which cannot penetrate to the individual organisms [50]. High concentrations of aminoglycosides may be necessary to effectively treat these organisms, as the positively charged antibiotic molecules may be bound up by the negatively charged polysaccharide matrix.
Multiple therapeutic modalities targeting airway infection must be employed in CF. Primary prevention with immunizations is extremely important for patients with CF. Viral respiratory infections have been shown to be both more severe in CF and to increase the likelihood of exacerbations of superimposed bacterial infection. The availability of measles vaccine and the corresponding decrease in severe measles pneumonia were major advances in CF care. Yearly, influenza vaccination and respiratory syncytial virus immunoprophylaxis in infancy are recommended. An effective vaccine for P. aeruginosa has not yet been developed but is a topic of active research [51, 52]. Because it is clear that there can be patient to patient transmission of bacteria, including P. aeruginosa and B. cepacia, strict infection control policies are in place at nearly all CF care centers [52–54].
Beyond prevention, it is recommended that all CF patients have their airways cultured routinely, approximately every 3 months, to monitor which pathogens are present. S. aureus is the predominant organism cultured early in life. Attempts at chronic suppression of this bacteria with daily antibiotics did not demonstrate a benefit to pulmonary function, but rather, chronic treatment increased the potential for earlier acquisition of P. aeruginosa [55, 56]. Earlier acquisition of P. aeruginosa corresponds with a more rapid decline in lung function; thus, significant attention in the CF community has been directed to ways to delay this milestone.
In most patients, intermittent recovery of P. aeruginosa precedes establishment of chronic infection (often defined as three consecutive positive cultures). Multiple studies have demonstrated that aggressive antibiotic treatment during the stage of intermittent infection may postpone chronic P. aeruginosa infection [57–58]. Currently, most CF care providers use daily inhaled antibiotics, which are rotated at monthly intervals to minimize the emergence of resistance [59, 60]. Most patients are also given systemic antibiotics (given orally or intravenously) for variable lengths of time.
Clinical Course and Treatment
Most patients with CF have a slow, progressive loss of pulmonary function over time, as a consequence of smoldering chronic infection and inflammation. This is punctuated by episodic exacerbations, which correspond with acquisition of new infectious agents (e.g., different bacteria, fungi, or mycobacteria) or sharp increases in the burden of bacteria and/or their invasiveness. Invasion of bacteria across the epithelium is frequently increased after the epithelium is damaged by viral infections, which are believed to be important triggers of exacerbations. During exacerbations, patients complain of increased cough and/or sputum production, fever, fatigue, weight loss, and occasionally chest pain, shortness of breath, and/or hemoptysis. They often experience transient but significant declines in pulmonary function and may have worsening of infiltrates on chest radiographs. When a pulmonary exacerbation becomes apparent, antibiotics tailored to the sensitivities of the cultured bacteria are prescribed [59]. These may be initiated empirically based on the results of the most recent surveillance cultures. The role and treatment of mycobacterial and fungal pulmonary infections are important but are beyond the scope of this review.
The majority of the bacteria are retained within the lumen of airways in CF. Tissue invasion, bacteremia, or serious infections outside of the sinopulmonary tract are rare. Therefore, inhaled antibiotics have an important role in CF (reviewed in [60]). Many drugs have been employed in this fashion, but tobramycin is the most extensively studied nebulized antibiotic in CF and is the most commonly used agent in the USA [61]. Inhaled antibiotics may be used intermittently for episodes of early infection with the goal of postponing chronic Pseudomonas infection. Later in the course of the disease, they are often used chronically in an alternating monthly regimen to reduce the bacterial burden. Inhaled therapy has the advantage of achieving high drug concentrations at the site of infection with minimal systemic absorption, thereby significantly reducing the potential for adverse effects. However, inhaled therapies can be irritating and cumbersome. The time required for inhalation of drugs and physical drainage sessions may take hours out of the CF patient’s (and parents’) day. Furthermore, delivery of drugs to the sites at which they are most needed is often limited by obstruction and impaired ventilation of densely involved airways.
In addition to inhaled antibiotics, aggressive systemic antibiotic treatment is necessary—by both oral and intravenous routes [59]. In some centers, intravenous antibiotics are administered routinely every few months in an effort to reduce bacterial burden within the airways. Antibiotics are given for greater duration and at significantly higher doses than would be given to patients without CF, based both on studies in CF patients demonstrating altered pharmocokinetics and on the need to achieve high concentrations within the airways [62–64]. Because of this, close clinical and biochemical monitoring is required.
Characteristics of Inflammation in CF Lung Disease
As previously stated, the histopathological process in the CF lung centers in and around the airways. Eventually, the enlarging, dense inflammatory exudate penetrates through the submucosa and involves the airway wall and supporting structures, leading to bronchiectasis. In contrast, the alveoli are relatively spared. Granulomas are rare, but the inflammatory mass, which eventually replaces the airways in CF, frequently contains lymphoid aggregates, which in some cases may even become organized into follicles and germinal centers [26].
At birth, the lungs of CF patients are structurally normal [25, 65]. However, plugging of the bronchioles with secretions and hypertrophy of submucosal gland ducts are seen by 4 months of age [65]. Once challenged by viral or bacterial infection, massive numbers of PMNs are persistently recruited to the airway. In normal individuals, the inflammatory response eradicates the infection and then is itself resolved. For example, PMNs that migrate into the airways usually phagocytose and kill the inciting bacteria, then undergo apoptosis, and are cleared by macrophages with little residual lung damage. This process fails in the CF airway for a number of reasons: (1) persistence of the bacteria provides a continuing pro-inflammatory stimulus; (2) there is a failure to turn off pro-inflammatory cytokine and chemokine production after an area is cleared of infection; and (3) many PMNs undergo necrosis rather than apoptosis, and there is impaired macrophage clearance of those which do enter apoptosis. A vicious cycle is established in which infection and inflammation lead to increased obstruction, creating more sites for persistent infection [66]. The progressive inflammation becomes a significant pathologic force, whose pernicious effects are responsible for much of the pathology in the CF lung and much of the morbidity and mortality suffered by the patients [27, 66].
The inflammation in the CF begins early, becomes persistent, and is excessive relative to the burden of infection [27–31]. BAL fluid from CF patients of all ages contains large concentrations of inflammatory mediators and massive amounts of PMNs and their products, including active elastase [27–31, 33–38, 66–70]. This is not surprising in adolescents and young adults, even those with mild disease and normal PFTs, because most of them are actually chronically infected [69]. However, cytokines, PMNs, and active elastase are present at impressive concentrations, even in CF infants [28–31, 35–37]. Moreover, these inflammatory markers are present, although at somewhat lower concentrations, in BAL fluid from apparently uninfected CF infants and young children who are not coughing [28, 29]. The presence of inflammation in the absence of detectable pathogens might suggest that the inflammatory response in the CF lung is autonomous and begins independently of an infectious stimulus. However, these findings may also be explained by failure to terminate the inflammatory response once the inciting stimulus has been eradicated. Thus, the presence of inflammatory cells and cytokines in the lungs of apparently un-infected CF babies may actually represent an abnormal persistence of inflammation after clearance of early, transient infection [38].
In addition to being abnormally persistent, several types of studies suggest that the inflammatory response in CF is also excessive relative to the burden of infection. BAL fluid from CF infants infected only with H influenzae contains more PMN and higher concentrations of the potent chemoattractant interleukin (IL)-8, for any given burden of bacteria, than does BAL fluid from infants with underlying conditions other than CF who are infected with the same organism [71, 72]. Similar comparisons show that CF BAL fluid contains more cytokines and PMN at any given concentration of LPS than BAL from other types of patients [73]. Animal and tissue culture experiments show that deficient CFTR function is associated with increased cytokine responses to a number of pro-inflammatory stimuli (see below). The huge excess of PMN release copious amounts of intracellular contents as they undergo necrosis. The sheer numbers of neutrophils exceed the ability of macrophages to clear them, and the ability of the macrophages to remove effete cells is also compromised. Long strands of uncleaved DNA and intact actin fibrils increase the viscosity of CF sputum and impair mucociliary clearance. These long molecules, which resist shear forces generated by ciliary action and cough, would normally be degraded during apoptosis. PMN also release oxidants and proteases, including elastase, which is often present in micromolar concentrations. Excessive amounts of oxidants overwhelm intra- and extracellular antioxidant defenses and contribute to lung injury [74–76]. The huge excess of elastase similarly overwhelms anti-proteases in the airways and results in uninhibited proteolytic enzyme activity [30, 66]. Elastase directly causes structural damage by digesting elastin and other airway wall proteins and worsens airway obstruction by impairing ciliary beating and increasing mucus secretion (reviewed in [66]). This enzyme is one of the most potent secretagogues known [77]. Recent studies also suggest that elastase can proteolytically activate the ENaC [78], which is believed to further exacerbate the abnormal Na+ resorption in the CF airway. Elastase also plays an important role in promoting bacterial persistence by cleaving critical opsonins such as iC3b and the Fc of IgG, as well as receptors such as CR1 and FcγRII, which are necessary for phagocytosis ([79] and reviewed in [66]). Similar cleavage of the phosphoserine receptor on macrophages is responsible for decreased clearance of those PMN, which do become apoptotic [80]. Elastase also promotes the generation of neutrophil chemoattractants, particularly IL-8, leukotriene (LT)B4, and C5a-like peptides from complement. Bacteria and their products also promote the generation of chemoattractants, which recruit more PMN into the airways, fueling the vicious cycle of inflammation, which leads to lung destruction (reviewed in [66]).
BAL fluid from patients with CF contains large concentrations of tumor necrosis factor-alpha (TNF-α), IL-1β, IL-6, and IL-8 [67, 71]. Excessive, dysregulated synthesis of these cytokines clearly contributes not only to the local pathology in CF but also to systemic manifestations of CF such as cachexia and hyperglobulinemia (reviewed in [66]). The intra- and intercellular mechanisms that contribute to the dysregulation of the inflammatory response will be discussed in the following sections of this review.
As one can see, defects in CFTR set in motion a vicious cycle of airway obstruction, infection that becomes difficult if not impossible to clear, and a heightened and prolonged inflammatory response within the lung. Unwanted consequences of the inflammation further contribute to poor airway clearance, destruction of the airways themselves, and ultimately to significant respiratory impairment and death. The remainder of this review will focus on the perturbations of cellular and intracellular pathways that result in the exaggerated inflammatory response in CF and on current efforts to understand and dampen this response therapeutically, with the goal of preserving lung function and prolonging life [81].
Disordered Intercellular Communication Results in Failure to Adequately Regulate the Inflammatory Response in the CF Lung
As the major morbidity and mortality in CF in the modern era is related to the chronic, destructive inflammatory process in the lung, many researchers have focused their efforts on understanding why the inflammation is so exuberant and how it escapes from normal control mechanisms. The lack of significant pulmonary inflammation at birth suggests that infection may initiate the inflammatory diathesis. However, the observations that babies in the first few months of life may have inflammation in the absence of detectable infection have suggested to some investigators that the infection may begin intrinsically, without any exogenous trigger. Some investigators have interpreted results of studies in CF cell lines as suggesting that mutations in Cftr, which cause retention of protein in the endoplasmic reticulum, lead to a “misfolded protein response,” causing epithelial cells to spontaneously produce inflammatory mediators [32]. However, other studies do not support this hypothesis.
Regardless of whether a low-grade inflammatory response may begin autonomously, most data support the idea that infection, even within the first few months of life, is an important stimulus that certainly exacerbates and perhaps initiates the excessive inflammation (reviewed in [34]). Studies in our own and other laboratories have focused on a failure to properly modulate and terminate the inflammatory response to infection, rather than abnormal initiation or activation of that response.
An important set of observations comes from serial studies of BAL fluid and bronchial epithelial cells from infants with CF before and after antibiotic therapy, which at that stage of the disease could successfully sterilize the lungs [33]. Findings of prolonged secretion of chemokines by bronchial epithelial cells, which persisted even after infection was eradicated, suggested the hypothesis that the presence of inflammatory mediators and higher numbers of PMN in the lungs of uninfected CF infants represents abnormal persistence of inflammation after clearance of early, transient infection [33]. In most acute inflammatory conditions, counter-regulatory mechanisms are upregulated shortly after activation of the inflammatory response and tend to return the host back to its baseline state quickly after the inciting stimulus (i.e., infection) is eradicated [82]. In CF, however, not only are the inflammatory mediators produced in excess, but termination of their production also seems impaired, as is apoptosis and removal of inflammatory cells (such as PMN) and their products.
Several investigators, going back many years, have reported increased levels of TNF-α in CF sputum, BAL, and serum. Pfeffer et al. reported in 1993 that macrophages from CF patients produced more TNF-α in response to lipopolysaccharide than similarly stimulated cells from normal controls [83]. Examinations of cytokines in CF BAL showed that CF airway secretions contain exorbitant concentrations of TNF-α, IL-1β, IL-6, and IL-8, PMNs, and PMN products [67, 71]. In contrast, the concentrations of counter-regulatory factors such as soluble TNF receptors and IL-1 receptor antagonist were only modestly increased, resulting in a marked excess of cytokine over inhibitor [67]. This contrasts with the situation found in BAL from normal controls, which showed marked excesses of inhibitors over the corresponding cytokines, TNF-α and IL-1β [83]. In addition, we and others have reported that the CF patients’ BAL contained relatively little IL-10 as compared to normal BAL [67, 83, 84]. This is potentially extremely important because IL-10 can suppress production of many pro-inflammatory cytokines and cellular responses.
The synthesis of many of the pro-inflammatory mediators whose concentrations are remarkably elevated in CF airway secretions is promoted by the transcription factor NF-κB. In addition, the transcription of other genes whose expression is also markedly elevated in the CF lung, such as ICAM-1 and Muc-5AC, are also increased by NF-κB. Studies of cell lines with impaired or inhibited CFTR show increased and prolonged activation of NF-κB in response to stimuli, as does lung tissue from cftr−/− mice. Possible intracellular reasons for this are discussed below, but potentially important contributors to increased NF-κB activation in vivo may include decreased IL-10 and/or decreased NO [85, 86].
IL-10 is an important anti-inflammatory and immunoregulatory cytokine. It can be produced by many cell types including macrophages, epithelial cells, T lymphocytes, and B lymphocytes. As noted above, airway secretions from CF patients and CF mice appear to be deficient in IL-10 as compared to airway secretions from normal individuals. This decrease in IL-10 is peculiar, as LPS and TNF-α, which are abundant in the CF airway, stimulate its production in normal subjects. IL-10 is constitutively expressed in normal airways [83]. Epithelial cells and/or dendritic cells are its likely source(s). The constitutive production of IL-10 could help to keep normal lungs free from inflammation. This is suggested by the observations that macrophages recovered from normal mouse or human lungs by BAL express little or none of the co-stimulatory molecules B7-1 or B7-2, and do not support T-cell activation in vitro [87]. In contrast, macrophages from the lungs of IL-10−/− (knockout) mice constitutively express both molecules, promote T-cell stimulation in vitro, and may increase antigen presentation in vivo [88]. This is important, as the large surface area of lung is exposed to thousands of antigens with each breath, and perpetual responses to such continuous stimulation would be undesirable. BAL macrophages from uninfected cftr−/− mice also show similar constitutive expression of B7-1 and B-7-2, and support T-cell proliferation [88]. These abnormalities can be reversed by treatment with exogenous IL-10, consistent with the suggestion that the CF airways may be deficient in IL-10 in vivo as a consequence of the basic defect in CFTR [88]. Studies demonstrating that stimulated peripheral blood T cells from CF patients produce less IL-10 than those from healthy subjects also support the idea that decreased IL-10 production is associated with the basic CF defect [89].
IL-10 normally serves to terminate acute inflammatory responses and promote their resolution by two main effects: downregulating production of pro-inflammatory cytokines and chemokines and by promoting PMN apoptosis [90]. In a state of relative IL-10 deficiency, initiation of apoptosis might be faulty, and PMN might survive longer and then undergo necrosis. Failure to activate nucleases and other degradative enzymes, which would normally be part of the apoptotic program [91], is likely the major reason why so much long stranded, rather than fragmented, DNA accumulates in the CF airways. This is one way in which decreased IL-10 would add to the persistence of PMN and their products in the CF airway. Normally, IL-10 turns off the production of NF-κB-dependent cytokines and other genes by several mechanisms, including increasing I-κB, the inhibitor of NF-κB [92, 93] and by destabilizing the mRNA for pro-inflammatory cytokines [94]. Thus, a failure to increase IL-10 production in response to LPS and other stimuli could contribute to persistence of chemokine and cytokine production after initial stimulation. NO, which is also surprisingly decreased in CF airways, normally increases I-κB as well [95] and thus would help to downregulate the acute inflammatory response. Thus, at least two important cut-off switches are impaired. Consequently, increased and persistent expression of NF-κB-dependent cytokines, chemokines, and adhesion molecules undoubtedly contribute to the persistent increase in PMN in the CF airways. With decreased levels of IL-10, NO, and other modulatory factors (see below) that should dampen the inflammatory response, the inflammation escapes from control and becomes like a freight train whose brakes have failed.
The impact of IL-10 deficiency on the inflammatory response to P. aeruginosa infection has been evaluated using several mouse models. First, IL-10−/− and cftr−/− mice have similar responses when acutely challenged with intratracheal LPS, a prototypic Toll-like receptor (TLR) agonist, which causes NF-κB activation and increases transcription of NF-κB-dependent genes [96]. Both types of mice had excessive pro-inflammatory cytokine production, prolonged and more profound depletion of IκB, and increased and persistent NF-κB activation after challenge, as compared to their wild-type (+/+) counterparts. These differences between cftr−/− and +/+ mice could be reversed by treating the cftr−/− mice with IL-10 before administering the LPS [96]. The effect of IL-10 deficiency on the intensity and duration of the inflammatory response to an acute, transient P. aeruginosa infection also has been studied in IL-10−/− and cftr−/− mice [97, 98]. After receiving an intratracheal inoculation of P. aeruginosa in free suspension (rather than in agarose beads-see below), IL-10−/− and cftr−/− mice both developed a more exuberant PMN response than +/+ mice. Both types of mice cleared the bacterial challenge over the same time interval, as compared to +/+ mice; but the increased numbers of PMN persisted after this in the IL-10−/− mice [97] and also in the cftr−/− mice [98]. This mimics the situation we reported in the CF infants who underwent serial BAL studies: inflammation persisted after the lungs had been cleared of bacteria. The excessive responses to LPS and to P. aeruginosa in both types of knockout mice were associated with enhanced pro-inflammatory cytokine and chemokine production, increased and prolonged NF-κB activation, and prolonged depletion of I-κBα, which was consumed in the initial phases of the lungs’ response to the acute challenge [97, 98]. The similarity of theses responses in IL-10−/− and cftr−/− mice and the normalization of the LPS response in cftr−/− mice when they were given exogenous IL-10 [96] strongly suggest that decreased IL-10 may contribute to the excessive and prolonged inflammatory response in CF.
A model, which has been very useful in CF research, is infection of animals with P. aeruginosa encased in agarose beads [99, 100]. The agarose beads stabilize the bacteria in the airways and prevent access of phagocytes to the individual organisms, thus inducing a chronic infection. Presumably, in this model, the effects of the agarose are analogous to those of the dehydrated mucus and the exopolysaccharide matrix of biofilm variants of P. aeruginosa. Histopathology of airways from animals infected in this way is very similar to that of airways from chronically infected CF patients [99]. Pilot studies of the effects of ibuprofen in this model in rats [101] paved the way for clinical trials of ibuprofen in CF patients. In the rats, treatment with that anti-inflammatory drug reduced the area of lung occupied by inflammatory exudates without increasing the burden of bacteria [101], supporting the suggestion that the inflammation in this model, as in CF, is greater than that required to control the infection per se. Infection of cftr−/− mice with P. aeruginosa in agar beads causes even further excesses in inflammation and increased weight loss and mortality as compared to similarly inoculated +/+ mice, although there was no dissemination of the infection and there were no differences in the burden of bacteria in the lungs [100]. As in the rats, in ibuprofen-treated patients, there was a slower rate of decline of lung function, with no increase in the apparent bacterial burden [102].
IL-10−/− mice inoculated with P. aeruginosa embedded in agarose beads had more drastic weight loss, greater PMN infiltration, larger amounts of the lung occupied by inflammatory exudates, and higher concentrations of pro-inflammatory cytokines in BAL than similarly infected +/+ mice [103]. Similarly inoculated cftr−/− mice, as compared to +/+ mice, had findings analogous to those seen in IL-10−/− mice, including more drastic weight loss, greater mortality, and increases in cytokine and chemokine production when compared to their +/+ controls [100]. In addition to its effect on the immediate inflammatory response, the absence of IL-10 may also result in long-term structural consequences. In a mouse model of chronic LPS exposure, the absence of IL-10 was associated with increased inflammatory cell infiltration and airway remodeling [104]. These effects were reversed by the administration of IL-10 [104]. It thus seems plausible that the imbalance between pro-inflammatory and anti-inflammatory cytokines plays an important role in some of the most prominent aspects of CF lung disease.
It has recently been reported that sputum of CF patients also contains elevated levels of IL-23 and IL-17 [105]. Studies comparing the agarose bead model of P. aeruginosa infection in IL-23p19−/− mice relative to +/+ mice show that in the absence of IL-23, there are decreases in the local concentrations of IL-17, the chemokine KC (a mouse homolog of IL-8), IL-6, and PMN, but no change in the bacterial burden or dissemination of infection [105]. These findings are again consistent with the idea that the use of the agarose beads, even in non-CF mice, induces an inflammatory response, which is similar to that in CF in being excessive relative to the burden of infection. In another series of studies, treatment of cftr−/− mice with neutralizing antibody to IL-17A reduced the excessive numbers of PMNs, other cells, and pro-inflammatory cytokines found in BAL after infection with P. aeruginosa in the agarose bead model [106]. Thus, IL-23, and the IL-17 it can induce, may play important roles in the excessive inflammation in CF in vivo, although their exact sources remain to be identified.
IL-6 is a pleiotropic cytokine, which has both pro- and anti-inflammatory activities. Additionally, IL-6 is generally considered to play a major role in inducing acute phase reactant production and in stimulating B-cell growth and function. Although it is clear that IL-6 is present in the CF airway in large concentrations, its role in this setting is unclear. Although initially felt to be a primarily pro-inflammatory cytokine, IL-6 can have anti-inflammatory properties as well. IL-6 induces IL-1 receptor antagonist and soluble TNF-α receptor synthesis and suppresses TNF-α and IL-1β transcription in human peripheral blood mononuclear cells [107–109]. Other evidence of IL-6’s anti-inflammatory effects comes from animal studies. Administration of IL-6 reduces TNF-α production and PMN influx and improves survival in some rodent models of infection, and the absence of IL-6 increases TNF-α and MIP-2 production and PMN influx in others [110–112]. It is certainly possible that IL-6 is exerting local anti-inflammatory effects in CF lung inflammation, but that these are overwhelmed by opposing pro-inflammatory influences. A priori, it would seem likely that IL-6 plays a role in the hyperglobulinemia found in most CF patients. On the other hand, however, most CF patients do not have elevated sedimentation rates or serum concentrations of C-reactive protein, which can be induced by IL-6. Signaling by the IL-6 receptor and its associated molecule gp130 proceeds through a pathway involving signal transducer and activator of transcription (STAT) [113]. STAT signaling may be disrupted in CF cells (see below), impairing the response to this cytokine. Clearly, further investigation into the role of IL-6 in the CF airway and its interaction with other mediators and cells is required.
Eicosanoids are products of arachidonic acid metabolism. Long considered important in CF airway pathophysiology, the eicosaonoids are a diverse family of arachidonic acid metabolites, which are potent regulators of inflammation and other physiologic responses. While leukotrienes and prostaglandins exert predominately pro-inflammatory effects, lipoxins primarily exert anti-inflammatory effects. LTB4, a potent neutrophil chemoattractant, is present in the CF airway in large concentrations [70]. Despite its instability in vitro in room air, the LTB4 concentrations of CF sputum and BAL samples may actually increase in vitro, due to active synthesis by the PMN and macrophages present. In contrast, lipoxin A4 (LXA4) is an important endogenous anti-inflammatory lipid mediator that promotes the resolution of acute neutrophilic inflammatory responses [114]. It has been reported that LXA4 concentrations are reduced in BAL fluid from stable CF patients as compared to non-CF inflamed controls [114]. Although the reasons for the decreased LXA4 concentrations have not been elucidated, administration of a metabolically stable lipoxin analog in a mouse model of chronic airway infection and inflammation decreased neutrophilic inflammation and disease severity without altering the infectious burden [114]. If verified in further pre-clinical studies, these data suggest that lipoxins may have potential therapeutic implications for CF and could be developed for future clinical trials. It is possible that another contributor to the putative imbalance between leukotrienes and lipoxins and other lipid mediators is an imbalance in the composition of the membrane lipids, which are the precursors of these mediators. CF cell lines, plasma and tissues of CF patients, and CF mice have been shown to have decreased docosoheaxnoic acid (DHA) and increased arachidonic acid in their membranes in their membranes [115]. Administration of supplemental DHA reversed the excessive inflammatory response to inhaled LPS in cftr−/− mice [116]. The agreement between findings in different experimental systems suggests that the alteration in the ratio of arachidonic acid to DHA may be directly related to defects in CFTR rather than being secondary to alterations in intestinal fat adsorption related to pancreatic insufficiency. The possibility that dietary manipulations may ameliorate disorders of inflammatory mediator production in CF certainly makes this an important subject of further investigation.
Defects in CFTR also impact production of NO, which can have regulatory and antimicrobial functions [117]. Exhaled NO is decreased in CF patients compared to non-CF patients [85, 86]. This is surprising, as exhaled NO is typically increased in inflammatory lung diseases [118]. Decreased NO may contribute in several ways to the pathophysiology of CF [117, 119–127]. First, decreased NO may adversely affect airway surface fluid by altering regulation of ion transport. When NO is decreased, sodium absorption by the airway epithelium is increased and chloride secretion is decreased, as is seen in CF [117]. Second, decreased NO impairs the ability of airway smooth muscle to relax in cftr−/− mice [119]. This may contribute to the bronchial obstruction seen in CF. Third, NO can potentiate oxidative anti-microbial mechanisms. NO can combine with superoxide to form the potent antimicrobial agent peroxynitrite, ONOO−. Peroxynitrite is more effective in killing B. cepacia complex organisms in vitro than either NO or \({\text{O}}_2^ - \) alone [120]. Oxidative mechanisms are probably more important in controlling this bacteria than in control of P. aeruginosa, which is not a particularly important pathogen in patients with chronic granulomatous disease. In addition, NO plays an important role in anti-viral defenses [124–127]. Hosts deficient in NO are more susceptible to viral infections. In CF, this is particularly important because viral infections are among the most important triggers for exacerbations of the chronic bacterial infection, and themselves can cause significant morbidity in CF. In vitro studies have shown that CF cells have decreased antiviral activity, presumably due to decreased interferon signaling (see below) and decreased induction of NO synthetase [121–125]. CF cell cultures are much more susceptible to cytopathologic effects of measles and influenza viruses and, failing to control the viruses, secrete more pro-inflammatory cytokines than similarly challenged non-CF cells [126, 127]. NO can have anti-inflammatory effects by stabilizing I-κB in macrophages (see below). Thus, decreased production of NO by epithelial and/or myeloid cells in CF likely makes important contributions not only to the increased propensity of CF patients to infection but also to the dysregulation of their inflammatory responses.
It thus seems quite clear that the inflammatory lung damage in CF is much more complicated than an exuberant response to a persistent pathogen. Although it is most likely that bacterial infection, particularly with mucoid P. aeruginosa, plays an important role in stimulating the inflammatory response in CF, it also seems clear that the inflammatory response itself is dysregulated in a number of important ways. These involve more than just over-production of any one family of pro-inflammatory mediators by a single type of cell. A variety of recent studies emphasize the concept that decreased anti-inflammatory and immunomodulatory activities are at least equally important as increases in pro-inflammatory mediators in shaping the overall pathophysiology of CF lung disease.
Disordered Intracellular Signaling and the Inflammatory Response in CF
Although the putative relation(s) between defects in CFTR and the abnormalities in intracellular signaling and resulting gene expression have not been clearly elucidated, there is considerable evidence suggesting a direct linkage, which is independent of interactions between different cell types and alterations in gastrointestinal adsorption or whole body disposition of lipids or other nutrients. Previous studies have shown that inhibition of CFTR production by antisense oligonucleotides and inhibition of CFTR function by over-expression of the regulatory (R) domain of CFTR both result in increased activation of NF-κB and increased secretion of IL-8 upon stimulation of epithelial cell lines with pro-inflammatory stimuli [128, 129]. This argues against a major problem related to an intracellular “misfolded protein” or “ER overload” response. Studies with a recently developed CFTR inhibitor also illuminate this question and support the idea that intact CFTR channel function per se is necessary for normal regulation of inflammatory cascades in epithelial cells [130]. Addition to cultured epithelial cell lines of the inhibitor “CFTRinh-172”, which putatively blocks the Cl− conductance of CFTR without otherwise altering its structure or function, caused increased IL-8 secretion in response to P. aeruginosa and to the combination of TNF-α and IL-1β [130]. This was accompanied by a number of alterations in intracellular signaling pathways characteristic of CF cells, including increased activation of NF-κB, increased expression of RhoA, and decreased expression of Smad3 (see below). There was no effect of this inhibitor on IL-8 production by cells that already lacked CFTR function, the effects were reversible upon withdrawal of the inhibitor, and there was no evidence of cytotoxicity [130]. These results provide a strong indication that alterations in the Cl− conductance of CFTR cause dysregulation of the intracellular signaling pathways.
As CFTR is itself an ion channel and modulates function of other channels, it seems natural to ask whether cells with defective CFTR expression or function have alterations in ion fluxes that mediate intracellular signals. Indeed, several investigators have shown that cells which lack adequate CFTR function are hyperpolarized and have increased Ca++ fluxes upon activation [131, 132]. A variety of ligand–receptor interactions stimulate Ca++ fluxes inside airway epithelial cells, including binding of bacteria to cell surface asialoGM1 glycolipids [129, 133]. Increased release of intracellular Ca++ stores and increased influxes of extracellular Ca++ likely both contribute to increased cytoplasmic free Ca++ [132, 133], which can increase activation of a number of protein kinase and other signaling pathways. These can contribute to increased pro-inflammatory responses, but the exact significance of epithelial cell Ca++ signaling in vivo is not clear, and whether CFTR defects alter Ca++ signaling in other types of cells remains a focus of active investigation. Defective cytokine production in epithelial cells, which are highly dependant on CFTR for normal secretory function, could explain why the disorders of the inflammatory response in CF seem limited to the respiratory tract. CFTR is expressed in lymphoblasts [135], but detection of the protein in mature myeloid or lymphoid cells is difficult to quantitate. Determination of the relative contributions of abnormalities in regulation of inflammatory signaling in myeloid vs epithelial cells is the subject of several lines of active investigation at the present time. Studies in (G551D) cftr−/− mice in which normal human CFTR was selectively expressed in particular cell types using transgenes with tissue-specific promoters suggested that defective CFTR function in the epithelium was necessary and sufficient to cause characteristic abnormalities in the response to LPS in the lung [136]. In contrast, studies using transplants of normal bone marrow into irradiated cftr−/− mice and of cftr−/− marrow into +/+ mice suggest that the genotype of the myeloid cells is more important than that of the intrinsic lung cells in determining the mortality from pseudomonas infection [137]. In agreement with those conclusions, recent studies have shown that transfection of normal human alveolar macrophages with adenoviral vectors containing siRNA, which suppresses CFTR expression, markedly increases their baseline and stimulated IL-8 production [138]. Clearly, further study is needed to determine the sites at which defects in CFTR critically alter the inflammatory response. Regardless of the extent to which signaling in myeloid and/or epithelial cells is affected, it seems likely that neither type of cell, alone, is responsible for all of the problems in the CF airway.
At least three major intracellular pathways, which regulate pro-inflammatory gene expression, are disturbed in CF epithelial cells: NF-κB, STATs, and PPAR. Although any of these individually might be expected to lead to dysregulation of production of extracellular signals that influence inflammation, exact predictions are difficult because there is a great deal of cross-talk between pathways, and gene transcription is rarely dependent on a single factor.
Because of the predominant roles of NF-κB-dependent cytokines and other NF-κB-dependent gene products in the pathophysiology of CF lung disease, this transcription factor and the pathways leading to its activation have received the most attention. Several Toll-like receptor and cytokine signaling pathways converge onto activation of I-κ kinase, which phosphorylates the cytoplasmic protein I-κB (for: inhibitor of NF-κB). This pathway thus integrates signals from multiple stimuli including LPS (via TLR4), flagellin (via TLR 5), and TNF-α and IL-1β (through MyD88 and upstream linkages to their individual receptors) [139–141]. I-κB normally holds NF-κB in an inactive complex in the cytoplasm. Phosphorylation of I-κB sets in motion a sequence of reactions in which I-κB detaches from NF-κB and becomes ubiquitinated and then degraded [139–141]. Results from our laboratory suggest that increased activation of I-κ kinase and/or failure to regenerate I-κB protein are key factors in the excessive activation of NF-κB in CF cells [96, 98]. Removal of the I-κB exposes a nuclear translocation sequence on NF-κB, which can then move into the nucleus and activate transcription of genes to whose promoters it binds [139–141]. The exact functions of NF-κB in the nucleus are further dependent on which NF-κB family member is involved (i.e., p65/p50, p65 dimers, etc.) and additional modifications such as acetylation and/or phosphorylation [139, 140]. Other transcription factors, particularly AP-1, are also involved in the regulation of expression of many of the same pro-inflammatory genes. Expression of the gene for I-κB itself is usually increased by NF-κB [142], providing a homeostatic feedback mechanism: increased production of I-κBα after NF-κB activation provides additional inhibitor, which helps to terminate the inflammatory reaction [141, 142]. The mechanisms by which this homeostatic mechanism is attenuated in CF continues to be a topic of active investigation.
Many inflammatory reactions are accompanied by increased production of NO, and measurement of increased concentrations of NO in exhaled breath has been advocated as a marker of inflammation in asthma [118]. It thus seems quite paradoxical that NO synthesis is actually decreased in CF. Studies aimed at understanding why the NO in CF is reduced have led to important insights into how intracellular signaling is dysregulated by defects in CFTR. In the normal lung and gastrointestinal tract, NO is constitutively produced by epithelial cells, but this is mostly the product of nitric oxide synthetase-2 (NOS-2), also known as inducible NOS (iNOS) [117, 121–123]. Although considered a pro-inflammatory or antimicrobial enzyme when it is induced in macrophages and other inflammatory cells, this enzyme is constitutively expressed in most epithelial cells, and it is responsible for most of the NO produced at mucosal surfaces [143]. Interestingly, NOS-2 expression in CF airway epithelial cells appears to be directly dependent on CFTR function [122, 123]. Cell lines in which CFTR function is inhibited by over-expression of the R-domain of CFTR have decreased expression of NOS-2 mRNA and NO [122]. In cells and tissues from CF patients and cftr−/− mice, epithelial production of NO is decreased and correlates with decreased expression of NOS-2 [121–123]. However, in the intestines (but not the airways) of cftr−/− mice who are additionally transgenic for the wild-type human cftr gene driven by an intestine-specific promoter, (so-called “gut corrected CF mice”) NOS expression is normalized [123]. Several studies suggest that constitutive NO production plays important roles in regulating epithelial ion transport and electrical potential and that reduction in NO production due to decreases in NOS activity are associated with increased Na+ readsorption and decreased Cl− permeability in CF [117, 123].
Decreased NO production may also lead to impairments in relaxation of bronchial smooth muscle, further contributing to airway obstruction in CF [119]. Although NOS2 expression is normally upregulated by NF-κB, maximal expression of this enzyme also requires interferon regulatory factor-1 (IRF-1). In turn, IRF-1 expression requires activation (phosphorylation) of STAT-1 [142]. Although CF cells contain normal amounts of STAT-1 and its phosphorylation does not seem to be impaired, the protein inhibitor of activated STAT-1 (PIAS-1) is also markedly upregulated [144]. This protein binds to phosphorylated STAT-1 and prevents its transcriptional activity, but the reasons why it is increased in CF remain to be determined. NOS2 expression is also regulated by the GTPase RhoA [145]. Increased RhoA has been reported in CF airway epithelial cells [145]. Manipulations of cultured cells, which result in increases in the active, GTP-bound form of RhoA, (such as deletion of proteins which activate its GTPase functions), lead to CF-like alterations in signaling intermediates, including decreased STAT-1 activation, increased PIAS-1, and impaired induction of NOS2 [145]. Rho is a prenylated molecule, and interference with synthesis of the isoprenoid moiety by mevastatin reverses these changes in cultured CF airway epithelial cells [146]. This interesting observation has clear therapeutic implications, which are being actively pursued. Observations of abnormalities in Rho GTPase function in CF cells due to changes in its prenylation prompted examination of another system of prenylated inflammatory regulators, which are also altered in CF, the Smad proteins [147]. These are small proteins that are associated in the cell membrane with TGF receptors but become translocated to the nucleus and modify gene transcription upon ligation of the receptor by TGF. The Smads then inhibit expression of IL-8 and other pro-inflammatory genes. CF phenotype cell lines and cells from CF mice have decreased Smad3 contents and decreased responses to TGF-β [147]. Inhibition of ispoprenoid transferases in these cellular models increases Smad3 protein levels and partially restores TGF-β mediated inhibition of IL-8 production. Obviously, any decrease in the activity of anti-inflammatory signaling pathways, like that of TGF-β, is potentially as important as any increase in pro-inflammatory signaling in a disease like CF.
Another set of intracellular controls, whose alterations in CF may contribute to increased pro-inflammatory gene expression, are the peroxisome proliferator activating receptor (PPAR) proteins [148–152]. These are nuclear receptors, which are members of the steroid hormone receptor family of ligand-activated transcription factors and exist in four isoforms (alpha, beta, gamma, and delta) [151]. When activated, PPAR forms a heterodimer with activated retinoid X receptor (RXR), which then modulates expression of multiple types of genes and has other intracellular activities [151, 152]. One of the major routes by which PPAR can attenuate inflammation is by inhibiting the actions of NF-κB by directly competing with its intranuclear binding sites that increase gene transcription [152]. PPAR also increases I-κB transcription, so any decrease in PPAR activity could contribute to the decreased I-κB replacement seen in CF cells and mouse tissues. PPARγ expression is decreased in lung, ileum, and colon of cftr−/− mice compared to +/+ littermates [150]. Furthermore, CF T cells and airway epithelial cell lines appear to have less PPAR activity than do non-CF T cells and airway epithelial cell lines [153, 154]. The widely used PPAR agonists troglitazone and ciglitazone activate PPAR in primary CF airway epithelial cells and CF epithelial cell lines, thereby inhibiting production of IL-8, IL-6, and granulocyte macrophage colony stimulating factor (GM-CSF) in response to incubation with P. aeruginosa [154]. Analogous results were obtained when cftr−/− mice were treated with the PPAR agonist pioglitazone [155]. Thus, decreased PPAR expression also likely contributes to the imbalance between I-κB and NF-κB that favors increased inflammation in CF, and widely used PPAR agonist drugs may have an important role in CF therapy.
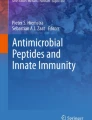
The mechanisms proposed above are not mutually exclusive. It is likely that a combination of the above intracellular processes result in abnormal extracellular signals, which fuel the aggressive and damaging inflammatory cascade. Figure 1 summarizes the effects of the documented abnormalities in CF.

Subcellular events associated with the documented abnormalities in cystic fibrosis. Decreased IL-10 and nitric oxide promote the degradation of I-κB in the airway epithelial cell and/or decrease its replacement. More NF-κB is activated, which promotes the transcription of the pro-inflammatory cytokines responsible for neutrophil dominated pathology. Decreased PPAR activation would further upregulate the inflammatory response by allowing persistent, unabated activity of NF-κB. As there are many triggers and products of the inflammatory response, therapeutics that exert their effects at the level of these signaling pathways would likely influence multiple pro-inflammatory mediators, and thus might be more effective than blockers of individual extracellular mediators
Anti-inflammatory Therapy in CF
CF is the most common genetic cause of early death in Caucasians, and inflammatory lung disease continues to be the major cause of morbidity and mortality [39]. As NF-κB-dependent cytokines and chemokines are major mediators of lung inflammation and destruction in CF, antagonists of the production and/or actions of these cytokines would be expected to be beneficial [27, 39, 81, 156]. Corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs), among other activities, increase I-κB concentrations and decrease NF-κB-dependent pro-inflammatory cytokine production [157, 158]. In animal models of chronic infection with P. aeruginosa in agarose beads, these agents caused reductions in area of lung sections occupied by PMN infiltrates and decreased lung inflammation and weight loss, without increasing the burden of bacteria or causing sepsis. Corticosteroids showed promising results in an early clinical trial [159], and in subsequent trials as well, there were no apparent infectious complications [160]. This tends to confirm the idea that the inflammatory response in CF is above and beyond what is necessary to control the infection. However, a subsequent large multicenter trial had to be stopped early due to adverse effects, including glucose intolerance [160]. Disturbingly, the use of prednisone resulted in decreased growth, which was not “made up” after the steroids were discontinued [161]. Trials of inhaled corticosteroids have not yielded conclusive results, perhaps because the drugs do not reach obstructed airways where they are needed most. A controlled clinical trial of ibuprofen showed significant decreases in the rate of decline of pulmonary function, higher weight scores, and decreased hospitalizations in the treated patients, again without apparent increases in the burden of infection or other signs of impaired host defenses [102]. However, occasional adverse effects such as gastrointestinal bleeding and nephrotoxicity (in combination with aminoglycosides), together with the need for closely monitored high doses and fears that these adverse effects will become widespread if the use of NSAIDs increases, have limited their use [162]. IL-10 showed effects similar to those of ibuprofen in mouse models [103] but has been withdrawn from human trials.
Reports that macrolide antibiotics have beneficial effects in a form of non-CF chronic pseudomonas pan-bronchiolitis prevalent in Japan [163] have prompted investigations into possible anti-inflammatory mechanisms of this class of drugs and clinical trials of azithromycin in CF. Subsequent studies indeed showed that macrolides decrease secretion of chemokines such as IL-8 and pro-inflammatory cytokines such as TNF-α in tissue culture and animal models, which do not depend on their antimicrobial activities [164–167]. The actual mechanisms of these effects and the relevance of individual mechanisms of action in vivo have not yet been fully elucidated, however. The results of a large, controlled multicenter trial in the USA showed better maintenance of pulmonary function, fewer exacerbations, and decreased requirements for full therapeutic courses of antibiotics in the azithromycin group [168]. Other studies have also shown decreased exacerbations in macrolide-treated patients, with or without significant differences in pulmonary function [169]. Some investigators caution that the chronic use of macrolides can select for resistant strains of S. aureus, but this has not seemed to cause clinical problems [170, 171].
Studies of inhibitors of individual chemokines or other mediators have shown promising results in vitro, but clinical trials have been disappointing, perhaps because of the multiplicity of mediator systems, which contribute to the over-exuberant inflammatory response in the CF lung. Clinical trials and animal studies to date are consistent in suggesting that anti-inflammatory agents can be effective in CF, at doses which will reduce the excessive response to infection, without impairing essential host defense activities. However, new therapies are needed, and an in-depth understanding of the dysregulated inflammatory response is a necessary prerequisite to identifying the most important targets and approaches for future research.
References
Tsui LC (1995) The cystic fibrosis transmembrane conductance regulator gene. Am J Respir Crit Care Med 151(3 Pt 2):S47–S53
Zielenski J, Tsui LC (1995) Cystic fibrosis: genotypic and phenotypic variations. Annu Rev Genet 29:777–807
Mickle JE, Cutting GR (2000) Genotype-phenotype relationships in cystic fibrosis. Med Clin North Am 84(3):597–607
Claustres M (2005) Molecular pathology of the CFTR locus in male infertility. Reprod Biomed Online 10(1):14–41
Cutting GR (2005) Modifier genetics: cystic fibrosis. Annu Rev Genomics Hum Genet 6:237–260
Drumm ML, Konstan MW, Schluchter MD (2005) Genetic modifiers of lung disease in cystic fibrosis. N Engl J Med 353:1443–1453
Hanrahan JW, Wioland MA (2004) Revisiting cystic fibrosis transmembrane conductance regulator structure and function. Proc Am Thorac Soc 1(1):17–21
Greger R, Mall M, Bleich M et al (1996) Regulation of epithelial ion channels by the cystic fibrosis transmembrane conductance regulator. J Mol Med 74:527–534
Kunzelmann K, Schreiber R, Nitschke R, Mall M (2000) Control of epithelial Na+ conductance by the cystic fibrosis transmembrane conductance regulator. Pflugers Arch 440:193–201
Jiang Q, Li J, Dubroff R, Ahn YJ et al (2000) Epithelial sodium channels regulate cystic fibrosis transmembrane conductance regulator chloride channels in Xenopus oocytes. J Biol Chem 275:13266–13274
Briel M, Greger R, Kunzelmann K (1998) Cl- transport by cystic fibrosis transmembrane conductance regulator (CFTR) contributes to the inhibition of epithelial Na+ channels (ENaCs) in Xenopus oocytes co-expressing CFTR and ENaC. J Physiol 508(Pt 3):825–836
Stutts MJ, Rossier BC, Boucher RC (1997) Cystic fibrosis transmembrane conductance regulator inverts protein kinase A-mediated regulation of epithelial sodium channel single channel kinetics. J Biol Chem 272:14037–14040
Hummler E, Barker P, Gatzy J et al (1996) Early death due to defective neonatal lung liquid clearance in alpha-ENaC-deficient mice. Nat Genet 12:325–328
Zahm JM, Baconnais S, Davidson DJ et al (2001) X-ray microanalysis of airway surface liquid collected in cystic fibrosis mice. Am J Physiol Lung Cell Mol Physiol 281:L309–L313
Jayaraman S, Joo NS, Reitz B et al (2001) Submucosal gland secretions in airways from cystic fibrosis patients have normal [Na(+)] and pH but elevated viscosity. Proc Natl Acad Sci U S A 98:8119–8123
Jayaraman S, Song Y, Vetrivel L et al (2001) Noninvasive in vivo fluorescence measurement of airway-surface liquid depth, salt concentration, and pH. J Clin Invest 107:317–324
Matsui H, Davis CW, Tarran R, Boucher RC (2000) Osmotic water permeabilities of cultured, well-differentiated normal and cystic fibrosis airway epithelia. J Clin Invest 105:1419–1427
Matsui H, Grubb BR, Tarran R et al (1998) Evidence for periciliary liquid layer depletion, not abnormal ion composition, in the pathogenesis of cystic fibrosis airways disease. Cell 95:1005–1015
Mall M, Grubb BR, Harkema JR et al (2004) Increased airway epithelial Na+ absorption produces cystic fibrosis-like lung disease in mice. Nat Med 10:487–493
Quinton PM (1999) Physiological basis of cystic fibrosis: a historical perspective. Physiol Rev 79(1 Suppl):S3–S22
Stern RC (1997) The diagnosis of cystic fibrosis. N Engl J Med 336(7):487–491
Bijman J, De Jonge H, Wine J (1988) Cystic fibrosis advantage. Nature 336(6198):430
Gabriel SE, Brigman KN, Koller BH, Boucher RC, Stutts MJ (1994) Cystic fibrosis heterozygote resistance to cholera toxin in the cystic fibrosis mouse model. Science 266(5182):107–109 (Oct 7)
Bedrossian CW, Greenberg SD, Singer DB et al (1976) The lung in cystic fibrosis. Hum Pathol 7:195–204
Sturgess J, Imrie J (1982) Quantitative evaluation of the development of tracheal submucosal glands in infants with cystic fibrosis and control infants. Am J Pathol 106:303–311
Tomashefski JF, Abramowsky CR, Dahms BB (1993) The pathology of cystic fibrosis. In: Davis PB (ed) Cystic fibrosis. Marcel Dekker, New York, pp 435–489
Konstan MW, Berger M (1997) Current understanding of the inflammatory process in cystic fibrosis: onset and etiology. Pediatr Pulmonol 24:137–142
Khan TZ, Wagener JS, Bost T et al (1995) Early pulmonary inflammation in infants with cystic fibrosis. Am. J Respir Crit Care Med 151:1075–1082
Armstrong DS, Hook SM, Jamsen KM et al (2005) Lower airway inflammation in infants with cystic fibrosis detected by newborn screening. Pediatr Pulmonol 40:500–510
Birrer P, McElvaney NG, Rudeberg A et al (1994) Protease-antiprotease imbalance in the lungs of children with cystic fibrosis. Am J Respir Crit Care Med 150:207–213
Cantin A (1995) Cystic fibrosis lung inflammation: early, sustained, and severe. Am J Respir Crit Care Med 151(4):939–941
DiMango E, Ratner AJ, Bryan R et al (1998) Activation of NF-kappaB by adherent Pseudomonas aeruginosa in normal and cystic fibrosis respiratory epithelial cells. J Clin Invest 101(11):2598–2605
Bonfield TL, Konstan MW, Berger M (1999) Altered respiratory epithelial cell cytokine production in cystic fibrosis. J Allergy Clin Immunol 104(1):72–78
Berger M (2002) Lung inflammation early in cystic fibrosis: bugs are indicted, but the defense is guilty. Am J Respir Crit Care Med 165(7):857–858
Balough K, McCubbin M, Weinberger M et al (1995) The relationship between infection and inflammation in the early stages of lung disease from cystic fibrosis. Pediatr Pulmonol 20(2):63–70
Armstrong DS, Grimwood K, Carzino R et al (1995) Lower respiratory infection and inflammation in infants with newly diagnosed cystic fibrosis. BMJ 310(6997):1571–1572
Armstrong DS, Grimwood K, Carlin JB et al (1997) Lower airway inflammation in infants and young children with cystic fibrosis. Am J Respir Crit Care Med 156(4 Pt 1):1197–1204
Chmiel JF, Konstan MW, Berger M (2002) The role of inflammation in the pathophysiology of CF lung disease. Clin Review Allergy Immunol 23(1):5–27
Davis PB, Drumm M, Konstan MW (1996) State of the art: Cystic fibrosis. Am J Resp Crit Care Med 154:1229–1256
CF Foundation Patient Registry Annual Data report (2005), CFF, Bethesda, MD, 2006
Quan JM, Tiddens HA, Sy JP et al (2001) A two-year randomized, placebo-controlled trial of dornase alfa in young patients with cystic fibrosis with mild lung function abnormalities. J Pediatr 139:813–820
McCoy K, Hamilton S, Johnson C (1996) Effects of 12-week administration of dornase alfa in patients with advanced cystic fibrosis lung disease. Chest 110:889–895
Hodson ME (1995) Aerosolized dornase alfa (rhDNase) for therapy of cystic fibrosis. Am J Respir Crit Care Med 151:S70–S74
Donaldson SH, Bennett WD, Zeman KL et al (2006) Mucus clearance and lung function in cystic fibrosis with hypertonic saline. N Engl J Med 354:241–250
Elkins MR, Robinson M, Rose BR et al (2006) A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis. N Engl J Med 354:229–240
Bauernfeind A, Bertele RM, Harms K et al (1987) Qualitative and quantitative microbiological analysis of sputa of 102 patients with cystic fibrosis. Infection 15:270–277
Gilligan PH (1991) Microbiology of airway disease in patients with cystic fibrosis. Clin Microbiol Rev 4:35–51
Donlan RM, Costerton JW (2002) Biofilms: survival mechanisms of clinically relevant microorganisms. Clin Microbiol Rev 15:167–193
Singh PK, Schaefer AL, Parsek MR et al (2000) Quorum-sensing signals indicate that cystic fibrosis lungs are infected with bacterial biofilms. Nature 407:762–764
Costerton JW, Lam J, Lam K, Chan R (1983) The role of the microcolony mode of growth in the pathogenesis of Pseudomonas aeruginosa infections. Rev Infect Dis 5(Suppl 5):S867–S873
Lang AB, Rudeberg A, Schoni MH et al (2004) Vaccination of cystic fibrosis patients against Psuedomonas aeruginosa reduces the proportion of patients infected and delays time to infection. Pediatr Infect Dis J 23:504–510
Zeurcher AW, Horn MP, Que JU et al (2006) Antibody responses induced by long-term vaccination with an octovalent conjugate Pseudomonas aeruginosa vaccine in children with cystic fibrosis. FEMS Immunol Med Microbiol 47:302–308
Festini F, Buzzetti R, Bassi C et al (2006) Isolation measures for prevention of infection with respiratory pathogens in cystic fibrosis: a systematic review. J Hosp Infect 64:1–6
Saiman L, Siegel J (2004) Infection control in cystic fibrosis. Clin Microbiol Rev 17:57–71
Stutman HR, Lieberman JM, Nussbaum E, Marks MI (2002) Antibiotic prophylaxis in infants and young children with cystic fibrosis: a randomized controlled trial. J Pediatr 140:299–305
Frederiksen B, Koch C, Hoiby N (1997) Antibiotic treatment of initial colonization with Pseudomonas aeruginosa postpones chronic infection and prevents deterioration of pulmonary function in cystic fibrosis. Pediatr Pulmonol 23:330–335
Wiesemann HG, Steinkamp G, Ratjen F et al (1998) Placebo-controlled, double-blind, randomized study of aerosolized tobramycin for early treatment of P. aeruginosa colonization in cystic fibrosis. Pediatr Pulmonol 25:88–92
Valerius NH, Koch C, Hoiby N (1991) Prevention of chronic P. aeruginosa colonization in cystic fibrosis by early treatment. Lancet 338:725–726
Gibson RL, Burns JL, Ramsey BW (2003) Pathophysiology and management of pulmonary infections in cystic fibrosis. Am J Respir Crit Care Med 168(8):918–951
Ryan G, Mukhopadhyay S, Singh M (2003) Nebulised anti-psuedomonal antibiotics for cystic fibrosis. Cochrane Database Syst Rev vol. 3. CD001021
Ramsey BW, Pepe MS, Quan JM et al (1999) Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl J Med 340:23–30
Spino M (1991) Pharmacokinetics of drugs in cystic fibrosis. Clin Rev Allergy 9:169–210
Touw DJ, Vinks AA, Mouton JW et al (1998) Pharmacokinetic optimization of antibacterial treatment in patients with cystic fibrosis: current practice and suggestions for future directions. Clin Pharacokinet 35:437–459
Rey E, Treluyer J, Pons G (1998) Drug disposition in cystic fibrosis. Clin Pharmacokinet 35:313–329
Bedrossian CW, Greenberg SD, Singer DB et al (1976) The lung in cystic fibrosis. A quantitative study including prevalence of pathologic findings among different age groups. Hum Pathol 7(2):195–204
Berger M (1991) Inflammation in the lung in cystic fibrosis. A vicious cycle that does more harm than good? Clin Rev Allergy Spring-Summer 9(1–2):119–142
Bonfield TL, Panuska JR, Konstan MW et al (1995) Inflammatory cytokines in cystic fibrosis lungs. Am J Respir Crit Care Med 152(6 Pt 1):2111–2118 [Published erratum appears in Am J Respir Crit Care Med 1996 Oct;154(4 Pt 1):1217]
Kirchner KK, Wagener JS, Khan TZ et al (1996) Increased DNA levels in bronchoalveolar lavage fluid obtained from infants with cystic fibrosis. Am J Respir Crit Care Med 154(5):1426–1429
Konstan MW, Hilliard KA, Norvell TM et al (1994) Bronchoalveolar lavage findings in cystic fibrosis patients with stable, clinically mild lung disease suggest ongoing infection and inflammation. Am J Respir Crit Care Med 150(2):448–454 [published erratum appears in Am J Respir Crit Care Med 1995 Jan:151(1)260]
Konstan MW, Walenga RW, Hilliard KA et al (1993) Leukotriene B4 is markedly elevated in the epithelial lining fluid of patients with cystic fibrosis. Am Rev Respir Dis 148(4 Pt 1):896–901
Noah TL, Black HR, Cheng PW et al (1997) Nasal and bronchoalveolar lavage fluid cytokines in early cystic fibrosis. J Infect Dis 175(3):638–647
Muhlebach MS, Stewart PW, Leigh MW et al (1999) Quantitation of inflammatory response to bacteria in young cystic fibrosis and control patients. Am J Respir Crit Care Med 160(1):186–191
Muhlebach MS, Noah TL (2002) Endotoxin activity and inflammatory markers in the airways of young patients with cystic fibrosis. Am J Respir Crit Care Med 165(7):911–915
Starosta V, Rietschel E, Paul K et al (2006) Oxidative changes of bronchoalveolar proteins in cystic fibrosis. Chest 129:431–437
Hull J, Vervaart P, Grimwood K, Phelan P (1997) Pulmonary oxidative stress response in young children with cystic fibrosis. Thorax 52:557–560
Kettle AJ, Chan T, Osberg I et al (2004) Myeloperoxidase and protein oxidation in the airways of young children with cystic fibrosis. Am J Respir Crit Care Med 170:1317–1323
Nadel JA (1991) Role of enzymes from inflammatory cells on airway submucosal gland secretion. Respiration 58(Suppl 1):3–5
Caldwell RA, Boucher RC, Stutts MJ (2005) Neutrophil elastase activates near-silent epithelial Na+ channels and increases airway epithelial Na+ transport. Am J Physiol Lung Cell Mol Physiol 288(5):L813–L819
Tosi MF, Zakem H, Berger M (1990) Neutrophil elastase cleaves C3bi on opsonized pseudomonas as well as CR1 on neutrophils to create a functionally important opsonin receptor mismatch. J Clin Invest 86(1):300–308
Vandivier RW, Fadok VA, Hoffmann PR et al (2002) Elastase-mediated phosphatidylserine receptor cleavage impairs apoptotic cell clearance in cystic fibrosis and bronchiectasis. J Clin Invest 109(5):661–670
Chmiel JF, Konstan MW (2005) Anti-inflammatory medications for cystic fibrosis lung disease: selecting the most appropriate agent. Treat Respir Med 4:255–273
Henson PM (1991) Resolution of inflammation. A perspective. Chest 99(3 Suppl):2S–6S
Bonfield TL, Konstan MW, Burfeind P et al (1995) Normal bronchial epithelial cells constitutively produce the anti-inflammatory cytokine interleukin-10, which is downregulated in cystic fibrosis. Am J Respir Cell Mol Biol 13(3):257–261
Osika E, Cavaillon JM, Chadelat K et al (1999) Distinct sputum cytokine profiles in cystic fibrosis and other chronic inflammatory airway disease. Eur Respir J 14(2):339–346
Balfour-Lynn IM, Laverty A, Dinwiddie R (1996) Reduced upper airway nitric oxide in cystic fibrosis. Arch Dis Child 75(4):319–322
Grasemann H, Michler E, Wallot M, Ratjen F (1997) Decreased concentration of exhaled nitric oxide (NO) in patients with cystic fibrosis. Pediatr Pulmonol 24(3):173–177
Chelen CJ, Fang Y, Freeman GJ et al (1995) Human alveolar macrophages present antigen ineffectively due to defective expression of B7 costimulatory cell surface molecules. J Clin Invest 95(3):1415–1421
Soltys J, Bonfield T, Chmiel J, Berger M (2002) Functional IL-10 deficiency in the lung of cystic fibrosis (cftr−/−) and IL-10 knockout mice causes increased expression and function of B7 costimulatory molecules on alveolar macrophages. J Immunol 168(4):1903–1910
Moss RB, Bocian RC, Hsu Y-P, Dong Y-J, Kemna M, Wei T et al (1996) Reduced IL-10 secretion by CD4+ T lymphocytes expressing mutant cystic fibrosis transmembrane conductance regulator (CFTR). Clin Exp Immunol 106(2):374–388
Cox G (1996) IL-10 enhances resolution of pulmonary inflammation in vivo by promoting apoptosis of neutrophils. Am J Physiol 271(4 Pt 1):L566–L571
Khodarev NN, Sokolova IA, Vaughan AT (1998) Mechanisms of induction of apoptotic DNA fragmentation. Int J Radiat Biol 73(5):455–467
Lentsch AB, Shanley TP, Sarma V, Ward PA (1997) In vivo suppression of NF-κB and preservation of IκBα by interleukin-10 and interleukin-13. J Clin Invest 100(10):2443–2448
Schottelius AJG, Mayo MW, Sartor RB, Baldwin AS Jr (1999) Interleukin-10 signaling blocks inhibitor of κB kinase activity and nuclear factor κB DNA binding. J Biol Chem 274(45):31868–31874
Hamilton TA, Ohmori Y, Tebo J (2002) Regulation of chemokine expression by antiinflammatory cytokines. Immunol Res 25(3):229–245
Welters ID, Fimiani C, Bilfinger TV, Stefano GB (2000) NF-kappaB, nitric oxide and opiate signaling. Med Hypotheses 54(2):263–268
Saadane A, Soltys J, Berger M (2005) Role of IL-10 deficiency in excessive nuclear factor-kappaB activation and lung inflammation in cystic fibrosis transmembrane conductance regulator knockout mice. J Allergy Clin Immunol 115(2):405–411
Chmiel JF, Konstan MW, Saadane A et al (2002) Prolonged inflammatory response to acute pseudomonas challenge in IL-10 knockout mice. Am J Respir Crit Care Med 165(8):1176–1181
Saadane A, Soltys J, Berger M (2006) Acute Pseudomonas challenge in cystic fibrosis mice causes prolonged nuclear factor-kappa B activation, cytokine secretion, and persistent lung inflammation. J Allergy Clin Immunol 117(5):1163–1169
Chmiel JF, Konstan MW, Berger M (2002) Murine models of CF airway infection and inflammation. Methods Mol Med 70:495–515
van Heeckeren A, Walenga R, Konstan MW et al (1997) Excessive inflammatory response of cystic fibrosis mice to bronchopulmonary infection with Pseudomonas aeruginosa. J Clin Invest 100(11):2810–2815
Konstan MW, Vargo KM, Davis PB (1992) Ibuprofen attenuates the inflammatory response Pseudomonas aeruginosa in a rat model of chronic pulmonary infection. Implications for anti-inflammatory therapy in cystic fibrosis. Am Rev Resp Dis 141:186–192
Konstan MW, Byard PJ, Hoppel CL, Davis PB (1995) Effect of high-dose ibuprofen in patients with cystic fibrosis. N Engl J Med 332:848–854
Chmiel JF, Konstan MW, Knesebeck JE et al (1999) IL-10 attenuates excessive inflammation in chronic pseudomonas infection in mice. Am J Respir Crit Care Med 160(6):2040–2047
Garantziotis S, Brass DM, Savov J et al (2006) Leukocyte-derived IL-10 reduces subepithelial fibrosis associated with chronically inhaled endotoxin. Am J Respir Cell Mol Biol 35(6):662–667
Dubin PJ, Kolls JK (2007) IL-23 mediates inflammatory responses to mucoid Pseudomonas aeruginosa lung infection in mice. Am J Physiol Lung Cell Mol Physiol Feb; 292(2):L519–L528. Epub 2006 Oct 27
Hsu DP, van Heeckeren A, Schlucter M et al (2006) IL-17 targeted antibody treatment increases the excessive pulmonary inflammation in CF mice. Pediatr Pulmonol Suppl 29:256
Tilg H, Trehu E, Atkins MB et al (1994) Interleukin-6 (IL-6) as an anti-inflammatory cytokine: induction of circulating IL-1 receptor antagonist and soluble tumor necrosis factor receptor p55. Blood 83(1):113–118
Jordan M, Otterness IG, Ng R et al (1995) Neutralization of endogenous IL-6 I suppresses induction of IL-1 receptor antagonist. J Immunol 154(8):4081–4090
Schindler R, Mancilla J, Endres S, Ghorbani R, Clark SC, Dinarello CA (1990) Correlations and interactions in the production of interleukin-6 (IL-6), IL-1, and tumor necrosis factor (TNF) in human blood mononuclear cells: IL-6 suppresses IL-1 and TNF. Blood 75(1):40–47
Ulich TR, Yin S, Guo K et al (1991) Intratracheal injection of endotoxin and cytokines. II. Interleukin-6 and transforming growth factor beta inhibit acute inflammation. Am J Pathol 138(5):1097–1101
Barton BE, Shortall J, Jackson JV (1996) Interleukins 6 and 11 protect mice from mortality in a staphylococcal enterotoxin-induced toxic shock model. Infect Immun 64(3):714–718
Xing Z, Gauldie J, Cox G, Baumann H (1998) IL-6 is an antiinflammatory cytokine required for controlling local or systemic acute inflammatory responses. J Clin Invest 101(2):311–320
Heinrich PC, Behrmann I, Haan S et al (2003) Principles of interleukin (IL)-6-type cytokine signalling and its regulation. Biochem J 374(Pt 1):1–20
Karp CL, Flick LM, Park KW, Softic S, Greer TM, Keledjia R et al (2004) Defective lipoxin-mediated anti-inflammatory activity in the cystic fibrosis airway. Nat Immunol 5(4):388–392
Freedman SD, Shea JC, Blanco PG, Alvarez JG (2000) Fatty acids in cystic fibrosis. Curr Opin Pulm Med 6(6):530–532
Freedman SD, Weinstein D, Blanco PG et al (2002) Characterization of LPS-induced lung inflammation in cftr−/− mice and the effect of docosahexaenoic acid. J Appl Physiol 92(5):2169–2176
Elmer HL, Brady KG, Drumm ML, Kelley TJ (1999) Nitric oxide-mediated regulation of transepithelial sodium and chloride transport in murine nasal epithelium. Am J Physiol 276(3 Pt 1):L466–L473
Kharitonov SA, Barnes PJ (2001) Exhaled markers of pulmonary disease. State of the art. Am J Respir Crit Care Med 163(7):1693–1722
Mhanna MJ, Ferkol T, Martin RJ et al (2001) Nitric oxide deficiency contributes to impairment of airway relaxation in cystic fibrosis mice. Am J Respir Cell Mol Biol 24(5):621–626
Smith AW, Green J, Eden CE, Watson ML (1999) Nitric oxide-induced potentiation of the killing of Burkholderia cepacia by reactive oxygen species: implications for cystic fibrosis. J Med Microbiol 48(5):419–423
Zheng S, Xu W, Bose S, Banerjee AK, Haque SJ, Erzurum SC (2004) Impaired nitric oxide synthase-2 signaling pathway in cystic fibrosis airway epithelium. Am J Physiol Lung Cell Mol Physiol 287(2):L374–L381
Kelley TJ, Drumm ML (1998) Inducible nitric oxide synthase expression is reduced in cystic fibrosis murine and human airway epithelial cells. J Clin Invest 102(6):1200–1207
Steagall WK, Elmer HL, Brady KG, Kelley TJ (2000) Cystic fibrosis transmembrane conductance regulator-dependent regulation of epithelial inducible nitric oxide synthase expression. Am J Respir Cell Mol Biol 22(1):45–50
Meng QH, Springall DR, Bishop AE et al (1998) Lack of inducible nitric oxide synthase in bronchial epithelium: a possible mechanism of susceptibility to infection in cystic fibrosis. J Pathol 184(3):323–331
Zheng S, Erzurum S (2001) Regulation of epithelial reactive oxygen and nitrogen species by inflammatory stimuli. Pediatr Pulmonol Suppl 12:128–129
Zheng S, De BP, Choudhary S, Comhair SA, Goggans T, Slee R et al (2003) Impaired innate host defense causes susceptibility to respiratory virus infections in cystic fibrosis. Immunity 18(5):619–630
Xu W, Zheng S, Goggans TM et al (2006) Cystic fibrosis and normal human airway epithelial cell response to influenza A viral infection. J Interferon Cytokine Res 26(9):609–627
Kube D, Sontich U, Fletcher D, Davis PB (2001) Proinflammatory cytokine responses to P. aeruginosa infection in human airway epithelial cell lines. Am J Physiol Lung Cell Mol Physiol 280(3):L493–L502
Bryan R, Kube D, Perez A, Davis P, Prince A (1998) Overproduction of the CFTR R domain leads to increased levels of asialoGM1 and increased Pseudomonas aeruginosa binding by epithelial cells. Am J Respir Cell Mol Biol 19(2):269–277
Perez A, Issler AC, Cotton CU et al (2006) CFTR inhibition mimics the cystic fibrosis inflammatory profile. J Physiol Lung Cell Mol Physiol 292:L383–L395
Machen TE (2006) Innate immune response in CF airway epithelia: hyperinflammatory? Am J Physiol Cell Physiol 291(2):C218–C230
Ribeiro CM, Paradiso AM, Carew MA et al (2005) Cystic fibrosis airway epithelial Ca2+ i signaling: the mechanism for the larger agonist-mediated Ca2+ i signals in human cystic fibrosis airway epithelia. J Biol Chem 280(11):10202–10209
Ratner AJ, Bryan R, Weber A et al (2001) Cystic fibrosis pathogens activate Ca2+ -dependent mitogen-activated protein kinase signaling pathways in airway epithelial cells. J Biol Chem 276(22):19267–19275
Tabary O, Boncoeur E, de Martin R et al (2006) Calcium-dependent regulation of NF-(kappa)B activation in cystic fibrosis airway epithelial cells. Cell Signal 18(5):652–660
McDonald TV, Nghiem PT, Gardner P, Martens CL (1992) Human lymphocytes transcribe the cystic fibrosis transmembrane conductance regulator gene and exhibit CF-defective cAMP-regulated chloride current. J Biol Chem 267(5):3242–3248
Oceandy D, McMorran BJ, Smith SN et al (2002) Gene complementation of airway epithelium in the cystic fibrosis mouse is necessary and sufficient to correct the pathogen clearance and inflammatory abnormalities. Hum Mol Genet 11(9):1059–1067
van Heeckeren AM, Davis PB (2004) Examining the contribution of resident and migratory cells in mediating the exaggerated inflammatory response in cystic fibrosis lung infections with mucoid P. aeruginosa. Pediatric Pulmonology Suppl. 27:274
Xu F, Krause A, Joh J et al (2006) Suppression of CFTR expression in alveolar macrophages enhances proinflamatory response to P. aeruginosa. Pediatr Pulmon Suppl 29:253
Karin M, Ben-Neriah Y (2000) Phosphorylation meets ubiquitination: The control of NF-κB activity. Ann Rev Immunol 18:621–663
Barnes PJ, Karin M (1997) NF-κB: A pivotal transcription factor in chronic inflammatory diseases. N Engl J Med 336:1066–1071
Scheidereit C (2006) IkappaB kinase complexes: gateways to NF-kappaB activation and transcription. Oncogene 25(51):6685–6705
Hoffmann A, Levchenko A, Scott ML, Baltimore D (2002) The IκB-NF-κB signaling module: temporal control and selective gene activation. Science 298:1241–1245
Guo FH, De Raeve HR, Rice TW et al (1995) Continuous nitric oxide synthesis by inducible nitric oxide synthase in normal human airway epithelium in vivo. Proc Natl Acad Sci U S A 92(17):7809–7813
Kelley TJ, Elmer HL (2000) In vivo alterations of IFN regulatory factor-1 and PIAS1 protein levels in cystic fibrosis epithelium. J Clin Invest 106(3):403–410
Kraynack NC, Corey DA, Elmer HL, Kelley TJ (2002) Mechanisms of NOS2 regulation by Rho GTPase signaling in airway epithelial cells. Am J Physiol Lung Cell Mol Physiol 283(3):L604–L611
Kreiselmeier NE, Kraynack NC, Corey DA, Kelley TJ (2003) Statin-mediated correction of STAT1 signaling and inducible nitric oxide synthase expression in cystic fibrosis epithelial cells. Am J Physiol Lung Cell Mol Physiol 285(6):L1286–L1295
Lee JY, Elmer HL, Ross KR, Kelley TJ (2004) Isoprenoid-mediated control of SMAD3 expression in a cultured model of cystic fibrosis epithelial cells. Am J Respir Cell Mol Biol 31(2):234–240
Zelvyte I, Dominaitiene R, Crisby M, Janciauskiene S (2002) Modulation of inflammatory mediators and PPARgamma and NFkappaB expression by pravastatin in response to lipoproteins in human monocytes in vitro. Pharmacol Res 45(2):147–154
Martin G, Duez H, Blanquart C et al (2001) Statin-induced inhibition of the Rho-signaling pathway activates PPARalpha and induces HDL apoA-I. J Clin Invest 107(11):1423–1432
Ollero M, Junaidi O, Zaman MM et al (2004) Decreased expression of peroxisome proliferators activated receptor gamma in cftr −/− mice. J Cell Physiol 200(2):235–244
Green S (1995) PPAR: A mediator of peroxisome proliferators action. Mutat Res 333(1–2):101–109
Vanden Berghe W, Vermeulen L, Delerive P (2003) A paradigm for gene regulation: inflammation, NF-kappaB, and PPAR. Adv Exp Med Biol 544:181–196
Reynders V, Loitsch S, Steinhauer C et al (2006) Peroxisome proliferator-activated receptor alpha (PPAR alpha) down-regulation in cystic fibrosis lymphocytes. Respir Res 7:104
Davis PB, Gupta S, Eastman J, Konstan MW (2003) Inhibition of proinflammatory cytokine production by PPARgamma agonists in airway epithelial cells. Pediatr Pulmonol Suppl 25:A246
van Heeckeren AM, Davis PB (2004) Effects of pioglitazone treatment in cystic fibrosis and wild type mice infected with Pseudomonas aeruginosa. Pediatric Pulmonology Suppl 28:237
Konstan MW, Davis PB (2002) Pharmacological approaches for the discovery and development of new anti-inflammatory agents for the treatment of cystic fibrosis. Adv Drug Deliv Rev 54:1409–1423
Auphan N, DiDonato A, Rosette C, Helmberg A, Karin M (1995) Immunosuppression by glucocorticoids: Inhibition of NF-κB activity through induction of IκB synthesis. Science 270:286–290
Yin MJ, Yamato Y, Gaynor RB (1998) The anti-inflammatory agents aspirin and salicylate inhibit the activity of IκB kinase-β. Nature 396:77–80
Auerbach HS, Williams M, Kirkpatrick JA, Colten HR (1985) Alternate-day prednisone reduces morbidity and improves pulmonary function in cystic fibrosis. Lancet 2:686–688
Eigen H, Rosenstein BJ, FitzSimmons S, Schidlow DV (1995) A multicenter study of alternate-day prednisone therapy to patients with cystic fibrosis. Cystic Fibrosis Foundation Prednisone Trial Group. J Pediatr 126:515–523
Lai HC, FitzSimmons SC, Allen DB et al (2000) Risk of persistent growth impairment after alternate-day prednisone treatment in children with cystic fibrosis. N Engl J Med 342(12):851–859
Oermann CM, Sockrider MM, Konstan MW (1999) The use of anti-inflammatory medications in cystic fibrosis. Chest 115:1053–1058
Keicho N, Kudoh S (2002) Diffuse panbronchiolitis: role of macrolides in therapy. Am J Respir Med 1(2):119–131
Abe S, Nakamura H, Inoue S et al (2000) Interleukin-8 gene repression by clarithromycin is mediated by the activator protein-1 binding site in human bronchial epithelial cells. Am J Respir Cell Mol Biol 22(1):51–60
Yamada T, Fujieda S, Mori S et al (2000) Macrolide treatment decreased the size of nasal polyps and IL-8 levels in nasal avage. Am J Rhinol 14(3):143–148
Cigana C, Nicolis E, Pasetto M, Assael BM, Melotti P (2006) Anti-inflammatory effects of azithromycin in cystic fibrosis airway epithelial cells. Biochem Biophys Res Commun 350(4):977–982
Equi AC, Davies JC, Painter H et al (2006) Exploring the mechanisms of macrolides in cystic fibrosis. Respir Med 100(4):687–697
Saiman L, Marshall BC, Mayer-Hamblett N et al (2003) Azithromycin in patients with cystic fibrosis chronically infected with Pseudomonas aeruginosa: a randomized controlled trial. JAMA 290(13):1749–1756
Saiman L (2004) The use of macrolide antibiotics in patients with cystic fibrosis. Curr Opin Pulm Med 10(6):515–523
Phaff SJ, Tiddens HA, Verbrugh HA, Ott A (2006) Macrolide resistance of Staphylococcus aureus and Haemophilus species associated with long-term azithromycin use in cystic fibrosis. J Antimicrob Chemother 57(4):741–746
Tramper-Stranders GA, Wolfs TF, Fleer A et al (2007) Maintenance azithromycin treatment in pediatric patients with cystic fibrosis: long-term outcomes related to macrolide resistance and pulmonary function. Pediatr Infect Dis J 26(1):8–12
Acknowledgments
Grant support from the National Institutes of Health Grant P30-DK27651 and the US Cystic Fibrosis Foundation is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nichols, D., Chmiel, J. & Berger, M. Chronic Inflammation in the Cystic Fibrosis Lung: Alterations in Inter- and Intracellular Signaling. Clinic Rev Allerg Immunol 34, 146–162 (2008). https://doi.org/10.1007/s12016-007-8039-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12016-007-8039-9