
Abstract
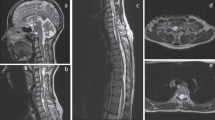
Horner syndrome (HS) results from the interruption of sympathic pathway, and the patients have a group of signs including miosis, ptosis, enophthalmos, and anhydrosis. While HS is mainly caused by cervical sympathetic nerve injury such as sympathetic chain tumor, we report here a HS case caused by a thoracolumbar arachnoid cyst. Imageological examination showed the cyst existed in spinal canal from the T11 to L3 level, which was further confirmed by operation. The tumor attacked the lateral margin of intervertebral foramen at certain stages. In MRI scan, no abnormality was found in the patient’s crania, cervical vertebra, thoracic vertebra, or the other parts. After removal of the cyst with operation, the patient’s HS symptoms and weakness of lower limbs were relieved apparently. Although the sympathetic center origins from the cornu laterale medullae spinalis of T1 to L3, there are many reports about HS caused by lumbar anesthesia and epidural anesthesia according to our literature review, and there is no report about HS results from intraspinal space-occupying lesion below T11 level. Our finding suggests that when the sympathetic center below the level of T11 emits nerve to dominate abdominal viscera, it can also control the sweat glands from face to feet, including pupils and eyelids. When physicians encounter patients with HS and one side of the body and abdominal viscera sympathetic syndromes, the pathological changes in lower thoracic vertebra or lumbar vertebra should be taken in consideration.





Similar content being viewed by others


References
Pirouzian, A., Holz, H. A., Ip, K. C., & Sudesh, R. (2010). Acquired infantile Horner syndrome and spontaneous internal carotid artery dissection: A case report and review of literature. Journal of AAPOS : The Official Publication of the American Association for Pediatric Ophthalmology and Strabismus/American Association for Pediatric Ophthalmology and Strabismus, 14, 172–174.
Syed, M. I., Baring, D., Addidle, M., Murray, C., & Adams, C. (2007). Lemierre syndrome: Two cases and a review. The Laryngoscope, 117, 1605–1610.
Kepes, E. R., Stark, D., Pantuck, E., et al. (1972). Horner’s syndrome following caudal anesthesia. New York State Journal of Medicine, 72, 946–947.
Clayton, K. C. (1983). The incidence of Horner’s syndrome during lumbar extradural for elective Caesarean section and provision of analgesia during labour. Anaesthesia, 38, 583–585.
Mohan, J., & Potter, J. M. (1975). Pupillary constriction and ptosis following caudal epidural analgesia. Anaesthesia, 30, 769–773.
Mohan, J., Lloyd, J. W., & Potter, J. M. (1973). Pupillary constriction following extradural analgesia. Injury, 5, 151–152.
Westermaier, T., Schweitzer, T., & Ernestus, R. I. (2012). Arachnoid cysts. Advances in Experimental Medicine and Biology, 724, 37–50.
Inagaki, T. (2011). Congenital anomalies in the central nervous system (12) arachnoid cyst. No shinkei geka. Neurological Surgery, 39, 1105–1111.
Greenberg, M. S., & Arredondo, N. (2006). Handbook of neurosurgery (6th ed.). Lakeland, FL, New York: Greenberg Graphics; Thieme Medical Publishers.
Fridman, A. (2004). Reversible Horner syndrome caused by solitary plasmacytoma of second thoracic vertebrae. Leukaemia & Lymphoma, 45(12), 2531–2532.
Acknowledgments
This work was supported by National Natural Science Foundation of China (Grant Nos. 81372869 and 81172555 to Y.G., Z.H., A.J., H.Z., and H.L.) and National Natural Science Fundation of Guangdong Province (Grant No. S2013010016052 to R.Z. and H.L.).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Yang Gao and Hui Zhang contributed equally as first authors.
Rights and permissions
About this article

Cite this article
Gao, Y., Zhang, H., Yang, J. et al. Thoracolumbar Arachnoid Cyst with Horner Syndrome: A Case Report and Review of the Literature. Cell Biochem Biophys 71, 1293–1297 (2015). https://doi.org/10.1007/s12013-014-0347-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12013-014-0347-0