
Abstract
Background
Burnout is common in professions such as medicine in which employees have frequent and often stressful interpersonal interactions where empathy and emotional control are important. Burnout can lead to decreased effectiveness at work, negative health outcomes, and less job satisfaction. A relationship between burnout and job satisfaction is established for several types of physicians but is less studied among surgeons who treat musculoskeletal conditions.
Questions/purposes
We asked: (1) For surgeons treating musculoskeletal conditions, what risk factors are associated with worse job dissatisfaction? (2) What risk factors are associated with burnout symptoms?
Methods
Two hundred ten (52% of all active members of the Science of Variation Group [SOVG]) surgeons who treat musculoskeletal conditions (94% orthopaedic surgeons and 6% trauma surgeons; in Europe, general trauma surgeons do most of the fracture surgery) completed the Global Job Satisfaction instrument, Shirom–Malamed Burnout Measure, and provided practice and surgeon characteristics. Most surgeons were male (193 surgeons, 92%) and most were academically employed (186 surgeons, 89%). Factors independently associated with job satisfaction and burnout were identified with multivariable analysis.
Results
Greater symptoms of burnout (β, −7.13; standard error [SE], 0.75; 95% CI, −8.60 to −5.66; p < 0.001; adjusted R2, 0.33) was the only factor independently associated with lower job satisfaction. Having children (β, −0.45; SE, 0.0.21; 95% CI, −0.85 to −0.043; p = 0.030; adjusted R2, 0.046) was the only factor independently associated with fewer symptoms of burnout.
Conclusions
Among an active research group of largely academic surgeons treating musculoskeletal conditions, most are satisfied with their job. Efforts to limit burnout and job satisfaction by optimizing engagement in and deriving meaning from the work are effective in other settings and merit attention among surgeons.
Level of Evidence
Level II, prognostic study.
Similar content being viewed by others


Introduction
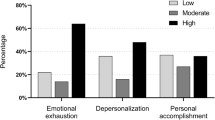
Burnout is a syndrome of depersonalization, emotional exhaustion, and a sense of low personal accomplishment that leads to decreased effectiveness at work [28]. Professions with intense involvement with people—including physicians [4, 10, 14, 27, 28] and nurses [13]—are prone to burnout. Job satisfaction however is thought to derive from intrinsic (eg, achievement and accomplishment) and extrinsic (eg, wages and job security) factors [23]. Greater job satisfaction among young surgeons is related to quality of care, patient satisfaction, and costs [24]. In a European study of surgical residents, only two-thirds were satisfied with their current working situation [32]. Factors that negatively affected trainee satisfaction were increasing work hours and perceived educational inadequacies. A previous study identified several factors that influence job satisfaction among young board-certified surgeons at academic centers in Europe and North America; ie, research opportunities, clinical autonomy, burnout, and work-life balance [24]. Younger surgeons, surgeons whose compensation was based entirely on billing or productivity, surgeons who worked more hours per week, and those who spent more nights on call were at greater risk. Subspecialists at greater risk were trauma, urology, otolaryngology, vascular, and general surgeons [26].
Orthopaedic and trauma surgeons perform invasive and often risky procedures to attempt to improve health, address limb- and life-threatening conditions, guide patients through rehabilitation, and help them regain confidence in their injured body. The work is rewarding but stressful. People who do stressful work build psychological and organizational resources to help manage the stress [15]. This can be difficult to maintain, and surgeons are susceptible to stress-related diseases (ie, depression and addiction), burnout, and dissatisfaction [5, 17, 30]. To help build and maintain resources to limit burnout and optimize job satisfaction among surgeons treating musculoskeletal conditions, it would help to have a better understanding of the associated factors. Therefore, we asked: (1) For surgeons treating musculoskeletal conditions, what risk factors are associated with worse job dissatisfaction? (2) What risk factors are associated with burnout symptoms?
Materials and Methods
This study was reviewed and approved by our institutional review board and a waiver of informed consent was obtained. All 707 email addresses in the database of the Science of Variation Group (SOVG) [9, 11] were used to invite participation in this 30-question online survey study (Appendix 1. [SurveyMonkey, Palo Alto, CA, USA]; Supplemental material is available with the online version of CORR ®) was used to create and conduct the survey. A reminder was sent after 2 weeks to those who did not respond. The SOVG consists of a group of orthopaedic and trauma surgeons who treat musculoskeletal problems (the majority of fracture treatment is done by general trauma surgeons in Europe) that studies variation in definitions, interpretations, and recommendations. There are groups of hand, trauma, shoulder, ankle, and general orthopaedic surgeons in the SOVG, all of whom treat fractures. The SOVG has 404 (57%) active members who responded to at least 20% of surveys to which they were invited. A total of 240 surgeons (59% of the active members) responded to the current survey. Seven surgeons (3%) responded to decline and 23 surgeons (10%) were excluded because they did not complete the whole questionnaire. Among the 210 surgeons who completed the survey, there were 198 (94%) orthopaedic surgeons and 12 (6%) trauma surgeons.
The primary outcome measure was the Global Job Satisfaction (GJS) instrument [16]. The GJS contains 12 items focusing on job satisfaction, which are scored on a scale ranging from −3 (strongly disagree) to 3 (strongly agree); such as, “I feel my current position is right for me.” For questions phrased negatively (questions 1, 2, 5, 6, 8, 10, and 12), scores were inverted: such as, “I feel stagnant in my position.” According to the GJS, a sum score greater than 0 indicates that a surgeon is satisfied with his or her current job, constituting a binary outcome variable (satisfied versus not satisfied). This validated questionnaire was created based on a sample of emergency department physicians in Canada [16, 24]. The survey was internally consistent in our sample (Cronbach’s α = 0.77). The mean GJS score was 17 with a standard deviation (SD) of ± 12, and 21 (10%) participants met the threshold (a sum score of ≤ 0) for dissatisfaction.
The secondary outcome was the Shirom–Malamed Burnout Measure (SMBM). The SMBM contains 14 statements, focusing on the individual’s feelings of physical, emotional, and cognitive exhaustion [29]. Items were scored answering the question “How often have you felt this way at work” on a seven-point Likert scale ranging from “never or almost never” to “always or almost always”; such as, “I feel tired.” A total score was calculated by taking the mean score of the 14 items, in which a higher score indicates more symptoms of burnout. A previous study, with a sample of 198 human service professionals, showed a Cronbach’s α of 0.92 [29]. The construct validity was assessed and compared with the Maslach Burnout Inventory–General Survey and superior results were found for the SMBM [29]. Several other studies used the SMBM to correlate burnout with physical health (eg, cardiovascular disease and type 2 diabetes) [20, 21, 31], thereby supporting its construct validity. We found substantial internal consistency (Cronbach’s α = 0.95) in our sample. The mean SMBM score was 2.5 with a SD of ± 0.98. The SBMS also was used as an explanatory variable when assessing factors associated with job satisfaction.
The member database of the SOVG was used to collect surgeon and practice characteristics: sex, area of practice, specialization, and supervising trainees. Additional characteristics were obtained through the survey; ie, years of independent practice, total number of publications, marital status, and number of children (Table 1).
Surveyed Population
A comparison was made between the surgeons who completed the survey (210 surgeons, 52%) and those who did not (194 surgeons, 48%); demographic data were missing for eight surgeons who did complete the survey. No differences were found in terms of sex (p = 0.68), practice location (p = 0.88), and years of independence practice (p = 0.63). A difference was found in subspecialties (general orthopaedics: 4% surveyed and 6% not surveyed; orthopaedic traumatology: 39% surveyed and 25% not surveyed; shoulder and elbow: 20% surveyed and 15% not surveyed; hand and wrist: 31% surveyed and 47% not surveyed; other: 14% surveyed and 14% not surveyed; p = 0.011) and surgeons who completed the survey were more likely to supervise surgical trainees (p = 0.014).
Statistical Analysis
Variables are presented as frequencies with percentages for categorical variables and mean with SD for continuous variables. Visual inspection of histograms suggested nonnormality of several continuous variables; however, there were no substantial outliers and the sample size was relatively large (n = 210). We therefore chose to describe the mean with SD for continuous variables and used parametric testing.
Bivariate analysis was used to assess the association between the explanatory variables and the outcome variable using an unpaired t-test for dichotomous explanatory variables, one-way ANOVA for the categorical variables, and Spearman’s rank correlation for the SMBM score. Variables with a p value less than 0.10 were included in a multivariable linear regression model to account for potential confounding. A two-sided p value less than 0.05 was considered significant. Categorical variables were dichotomized when included in the multivariable analysis.
Results
After accounting for the potential confounding variable (ie, number of children) (Table 2), we found that only greater symptoms of burnout (β, −7.13; standard error [SE], 0.75; 95% CI, −8.60 to −5.66; p < 0.001; adjusted R2, 0.33) was independently associated with lower job satisfaction (Table 3). After accounting for potential confounding variables such as sex and years of independent practice (Table 4), we found that only having children (β, −0.45; SE, 0.0.21; 95% CI, −0.85 to −0.043; p = 0.030; adjusted R2, 0.046) was independently associated with fewer symptoms of burnout (Table 5).
Discussion
Burnout is known to occur in professions with frequent, stressful interpersonal interactions and can lead to decreased effectiveness at work, negative health outcomes, and less job satisfaction [5, 17, 18, 30]. A relationship between burnout and job satisfaction is established for several types of physicians [1, 4, 8, 10, 14, 19, 26, 27], but has been studied less among surgeons treating musculoskeletal conditions. To be able to build and maintain resources to address these issues, it would help to have a better understanding of job satisfaction and burnout among this group of surgeons. Therefore, we asked: (1) For surgeons treating musculoskeletal conditions, what risk factors are associated with worse job dissatisfaction? (2) What risk factors are associated with burnout symptoms?
This study has some limitations. First, this study was designed as a cross-sectional study, which allows identifying relationships between variables at one time point only but does not allow identifying causal associations. To get a better understanding of the development of burnout with time, a longitudinal study is necessary. Second, our survey completion rate (51%) is lower than physician surveys in general [6, 12] and this could introduce response bias. It is not known if physicians who are burnt out are less likely to participate owing to apathy or more likely owing to greater interest in the subject. A comparison between the surgeons who completed the survey and those who did not showed that there were more academically employed surgeons who completed the survey. The groups were similar in terms of sex, years of independent practice, and practice location, probably keeping the response bias to a minimum. Our sense is that some surgeons are more likely to volunteer their time for these surveys and that what we learn from the surveys applies best to the reliable responders. The third limitation is that all measures are based on self-reports. This may cause measurement bias, although there is an argument that because stress is an experience based on perception, subjective report has to be paramount. Fourth, of the 210 participants, only 21 (10%) were not satisfied with their job. This could make a multivariable model, depending on the number of variables included, less reliable. However, we did not include more than four variables in our multivariable model, which is still within reasonable limits and which maintains the reliability. Fifth, given that 89% of participants supervise trainees, the results are most applicable to academically employed surgeons treating musculoskeletal conditions than to community surgeons. There may be other important differences between participants and the average surgeon that we did not account for. Nevertheless, the finding that job dissatisfaction is related to burnout seems likely to hold in different populations although there might be differences in the prevalence and magnitude of burnout and dissatisfaction. Finally, the GJS has a yes or no outcome. This makes it impossible to discriminate between surgeons in the not satisfied and satisfied groups. A continuous scale would allow for more detailed analysis.
The only factor associated with a decrease in job satisfaction was greater symptoms of burnout. Our finding that job satisfaction correlates with burnout is consistent with the results of the study by Raptis et al. [24]. Raptis et al. studied factors influencing job satisfaction of North American and European academic surgeons in their first 10 years after board certification and found 83% and 85% of the surgeons were satisfied with their jobs, respectively. A North American study of trauma surgeons found a 40% prevalence of burnout rated categorically and also found burnout to explain most of the variation in job dissatisfaction. Seventy percent of the surgeons (only 2% of them orthopaedic surgeons) would choose to become a surgeon again [26]. A study of burnout among academic orthopaedic department chairmen found moderate levels of emotional exhaustion and depersonalization [25]. In another study of academic surgeons in 14 different surgical specialties, orthopaedic surgeons (155 participants) were found to have one of the lowest risks of burnout (32%) [3]. Similar to orthopaedic trauma surgeons [7] but contrary to other surgical specialties [3, 19], the personal lives (ie, marital status and number of children) of the surgeons did not seem to influence their job satisfaction in our study.
The only factor in our study that was associated with burnout was number of children. In the study by Balch et al. [2] looking at North American surgeons, the number of hours worked and the number of nights on call were strongly related to burnout. The lack of questions addressing hours worked and nights on call in our study might explain the relatively small proportion (R2, 0.046) of variance in burnout accounted for in our model. Prior studies of North American surgeons showed an association between being a parent and a decrease in burnout risk [22, 26]. Perhaps surgeons who consider having children feel more stable professionally and less prone to burnout or perhaps a more enriching family life and work-life balance are protective. The lower burnout risk might be explained by the relative healthy patient population and relative good survival of most orthopaedic patients. It has been suggested that physicians who see chronically ill patients in their clinic are at higher risk for burnout [3].
Treating orthopaedic patients in an academic setting is rewarding, with 90% of all surgeons being satisfied with their jobs. Job dissatisfaction is associated with burnout although it is unclear if this is a unidirectional or bidirectional relationship. It seems important to develop strategies to recognize and mitigate symptoms of burnout in the workplace and create and maintain resources that can address these issues.
References
Ahmadiyeh N, Cho NL, Kellogg KC, Lipsitz SR, Moore FD Jr, Ashley SW, Zinner MJ, Breen EM. Career satisfaction of women in surgery: perceptions, factors, and strategies. J Am Coll Surg. 2010;210:23–28.
Balch CM, Shanafelt TD, Dyrbye L, Sloan JA, Russell TR, Bechamps GJ, Freischlag JA. Surgeon distress as calibrated by hours worked and nights on call. J Am Coll Surg. 2010;211:609–619.
Balch CM, Shanafelt TD, Sloan JA, Satele DV, Freischlag JA. Distress and career satisfaction among 14 surgical specialties, comparing academic and private practice settings. Ann Surg. 2011;254:558–568.
Bertges Yost W, Eshelman A, Raoufi M, Abouljoud MS. A national study of burnout among American transplant surgeons. Transplant Proc. 2005;37:1399–1401.
Brooks SK, Chalder T, Gerada C. Doctors vulnerable to psychological distress and addictions: treatment from the Practitioner Health Programme. J Ment Health. 2011;20:157–164.
Cho YI, Johnson TP, Vangeest JB. Enhancing surveys of health care professionals: a meta-analysis of techniques to improve response. Eval Health Prof. 2013;36:382–407.
Cunningham BP, Swanson D, Basmajian H, McLemore R, Ortega G. Professional demands and job satisfaction in orthopaedic trauma: an OTA member survey. J Orthop Trauma. 2015;29:e499–503.
DeVoe J, Fryer GE Jr, Hargraves JL, Phillips RL, Green LA. Does career dissatisfaction affect the ability of family physicians to deliver high-quality patient care? J Fam Pract. 2002;51:223–228.
Guitton TG, Ring D; Science of Variation Group. Interobserver reliability of radial head fracture classification: two-dimensional compared with three-dimensional CT. J Bone Joint Surg Am. 2011;93:2015–2021.
Guntupalli KK, Fromm RE Jr. Burnout in the internist: intensivist. Intensive Care Med. 1996;22:625–630.
Hageman MG, Guitton TG, Ring D; Science of Variation Group. How surgeons make decisions when the evidence is inconclusive. J Hand Surg Am. 2013;38:1202–1208.
Kellerman SE, Herold J. Physician response to surveys: a review of the literature. Am J Prev Med. 2001;20:61–67.
Kilfedder CJ, Power KG, Wells TJ. Burnout in psychiatric nursing. J Adv Nurs. 2001;34:383–396.
Kuerer HM, Eberlein TJ, Pollock RE, Huschka M, Baile WF, Morrow M, Michelassi F, Singletary SE, Novotny P, Sloan J, Shanafelt TD. Career satisfaction, practice patterns and burnout among surgical oncologists: report on the quality of life of members of the Society of Surgical Oncology. Ann Surg Oncol. 2007;14:3043–3053.
Larsen A, Boggild H, Mortensen JT, Foldager L, Hansen J, Christensen A, Arendt M, Rosenberg N, Munk-Jorgensen P. Psychopathology, defence mechanisms, and the psychosocial work environment. Int J Soc Psychiatry. 2010;56:563–577.
Lloyd S, Streiner D, Hahn E, Shannon S. Development of the emergency physician job satisfaction measurement instrument. Am J Emerg Med. 1994;12:1–10.
Mache S, Vitzthum K, Klapp BF, Danzer G. Surgeons’ work engagement: influencing factors and relations to job and life satisfaction. Surgeon. 2014;12:181–190.
Maslach C, Schaufeli WB, Leiter MP. Job burnout. Ann Rev Psychol. 2001;52:397–422.
McAbee JH, Ragel BT, McCartney S, Jones GM, Michael LM 2nd, DeCuypere M, Cheng JS, Boop FA, Klimo P Jr. Factors associated with career satisfaction and burnout among US neurosurgeons: results of a nationwide survey. J Neurosurg. 2015;123:161–173.
Melamed S, Shirom A, Toker S, Berliner S, Shapira I. Burnout and risk of cardiovascular disease: evidence, possible causal paths, and promising research directions. Psychol Bull. 2006;132:327–353.
Melamed S, Shirom A, Toker S, Shapira I. Burnout and risk of type 2 diabetes: a prospective study of apparently healthy employed persons. Psychosom Med. 2006;68:863–869.
Qureshi HA, Rawlani R, Mioton LM, Dumanian GA, Kim JY, Rawlani V. Burnout phenomenon in U.S. plastic surgeons: risk factors and impact on quality of life. Plast Reconstr Surg. 2015;135:619–626.
Rafferty JP, Lemkau JP, Purdy RR, Rudisill JR. Validity of the Maslach Burnout Inventory for family practice physicians. J Clin Psychol. 1986;42:488–492.
Raptis DA, Schlegel A, Tschuor C, Clavien PA. Job satisfaction among young board-certified surgeons at academic centers in Europe and North America. Ann Surg. 2012;256:796-803; discussion 803–800.
Saleh KJ, Quick JC, Conaway M, Sime WE, Martin W, Hurwitz S, Einhorn TA. The prevalence and severity of burnout among academic orthopaedic departmental leaders. J Bone Joint Surg Am. 2007;89:896–903.
Shanafelt TD, Balch CM, Bechamps GJ, Russell T, Dyrbye L, Satele D, Collicott P, Novotny PJ, Sloan J, Freischlag JA. Burnout and career satisfaction among American surgeons. Ann Surg. 2009;250:463–471.
Shanafelt TD, Balch CM, Bechamps G, Russell T, Dyrbye L, Satele D, Collicott P, Novotny PJ, Sloan J, Freischlag J. Burnout and medical errors among American surgeons. Ann Surg. 2010;251:995–1000.
Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136:358–367.
Shirom A, Melamed S. A comparison of the construct validity of two burnout measures in two groups of professionals. Int J Stress Manag. 2006;13:176–200.
Shirom A, Westman M, Shamai O, Carel RS. Effects of work overload and burnout on cholesterol and triglycerides levels: the moderating effects of emotional reactivity among male and female employees. J Occup Health Psychol. 1997;2:275–288.
Toker S, Melamed S, Berliner S, Zeltser D, Shapira I. Burnout and risk of coronary heart disease: a prospective study of 8838 employees. Psychosom Med. 2012;74:840–847.
von Websky MW, Oberkofler CE, Rufibach K, Raptis DA, Lehmann K, Hahnloser D, Clavien PA. Trainee satisfaction in surgery residency programs: modern management tools ensure trainee motivation and success. Surgery. 2012;152:794–801.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Science of Variation Group
A. Peters; A.B. Spoor; A.D. Armstrong; J. Abboud; A. Shrivastava: A.L. Wahegaonkar; A. Chauhan; A.B. Shafritz; J. Adams; A.E. Garcia G.; A.J.H. Vochteloo; A.J. Powell; A. Platz; A.N. Miller; A. Barquet; A. Kristan; A. Berner; A.S. Ranade: A. Jubel; B.J. Cross; B.E. Kreis; T. Bafus; B. Bamberger; B. Sutker; F.L. Walter; J. Braman; B.P.D. Wills; H. Broekhuyse; R. Buckley; B.W. Sears; R.P. Calfee; C. Ekholm; C.H. Fernandes; C. Swigart; C. Cassidy C.D. Oliveira Miranda; C. Taleb; G. Porcellini; C.L. Moreno-Serrano; C. Lomita; C. Manke; C.M. Jones; B.D. Crist; M.A. Pirela-Cruz; C. Klostermann; D.F.P. van Deurzen; D. Beingessner; D. Drosdowech; G.J. Della Rocca; D. Eygendaal; D. Polatsch; C.J. Romero Barreto; M. Merchant; D. Brilej; N. Bijlani; E. Maman; D.A. Rikli; M. Shafi; J.M. Patiño; R. van Riet; S.F. Duncan; E.F. Ibrahim; E.G. Ballas; E. Melamed; E. Stojkovska Pemovska; E.T. Walbeehm; P.J. Evans; F. Suarez; F. Frihagen; F. Lopez-Gonzalez; C. Garnavos; G. DeSilva; G.S.M. Dyer; G.C. Babis; G. Kohut; G. Kontakis; G. Panagopoulos; C.A. Goldfarb; G.J. Bayne; G. Merrell; G.R. Hernandez; H.W. Grunwald; T.G. Guitton; L.A. Campinhos; J.Hall; M. Nancollas; C. Young; L.B. Lane; I. Pountos; E. Hofmeister; H. Durchholz; I. McGraw; I. Harris; I.F. Kodde; L. Marsh; J. Biert; J. Bishop; J.M. Abzug; J.E. Kazanjian; J.A. Greenberg; J.A. Gillespie; J.C. Fanuele; J. Choueka; J.E. Ribeiro Filho; J. Itamura; J.M. Conflitti; J. Miguel; R. Roiz; J.M. Wiater; J. Nolla; J.H. Scheer; J. Rubio; S. Kakar; M.D. Kaminaris; K. Chivers; K. Egol; K. Jeray; K.J. Prommersberger; K.M. Rumball; K. Kabir; G.A. Kraan; K. Dickson; L.M.S.J. Poelhekke; L. Mica; L.E. Adolfsson; L.C. Borris; N.G. Lasanianos; L.M. Schulte; L. Elmans; L. Paz; L.F. Naquira Escobar; L.S. Austin; M. Mormino; M.J. Richard; M. Di Micoli; M. Bonczar; M.I. Loebenberg; E.M. Hammerberg; M. Menon
J. McAuliffe; M. Mckee; M. Soong; M/ Darowish; M.M. Wood; MI. Abdel-Ghany; M. Quell; M.W. Kessler; M. Patel; M.J. Palmer; M. Prayson; M.S. Karamitopoulos; M. Pirpiris; M. Tyllianakis; M.W. Grafe; N. Elias; N.M. Akabudike; N.L. Shortt; N. Rossiter; N.K. Kanakaris; J.T. Capo; O. Brink; R. Omid; M. Richardson; J.A. Ortiz; J.W. Johnson; P.V. van Eerten; P. Inna; P. Dantuluri; P. Paladini; P. Althausen; P. Appleton; P. Sancheti; N. Parnes; P.A. Martineau; P. Blazar; P. Krause; P. Schandelmaier; P. Jebson; P. Levin; W. Arnnold Batson; L. Guenter; R.W. Peters; R.M. Ramli; R. de Bedout; S. Rowinski; R.H. Babst; R.R.L. Gray; R. Papandrea; R.S. Gilbert; M. Rizzo; R. Jenkinson; R.M. Smith; R.D. Zura; R.S. Page; R. Pesantez; D. Ruch; R. Wagenmakers; J. Abrams; S.H. van Helden; V.J. Sabesan; S.A. Kennedy; S. Bouaicha; S. Beldner; S. Mitchell; S. Dodds; B.M. Nolan; S. Hurwit; S. Kaplan; S.G. Kaar; S.A. Meylaerts; T. Omara; M. Swiontkowski; T. Gosens; T. Schepers; T. DeCoster; L. Taitsman; T. Baxamusa; T. Dienstknecht; F.T.D. Kaplan; T. Siff; T. Begue; T. Mittlmeier; T. Apard; T. Chesser; T.J. Fischer; T. Havlicek; T. Wyrick; T. Tosounidis; V. Giordano; T.F. Varecka; V.S. Nikolaou; V. Philippe; C.J. Walsh; W.C. Hammert; M. Waseem; Y. Weil; W. Satora; C. Zalavras; J. Fischer
One of the authors certifies that he (DR) has received payments, during the study period, of less than USD 10,000 from Tornier (formerly Wright Medical), (Bloomington, IN,
USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
This work was performed at Massachusetts General Hospital, Boston, MA, USA.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
van Wulfften Palthe, O.D.R., Neuhaus, V., Janssen, S.J. et al. Among Musculoskeletal Surgeons, Job Dissatisfaction Is Associated With Burnout. Clin Orthop Relat Res 474, 1857–1863 (2016). https://doi.org/10.1007/s11999-016-4848-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-016-4848-6