
Abstract
Background
The early recovery period after periacetabular osteotomy (PAO) can be limited by pain and activity restrictions. Modifications of the Bernese PAO, including sparing the rectus tendon and discontinuing routine arthrotomy, may accelerate early postoperative recovery compared with the standard approach.
Questions/purposes
Does a modified approach for PAO (1) lead to improved pain control immediately after surgery; (2) lead to improved ambulation during the hospital stay; (3) lead to shorter stays, less blood loss, and shorter surgical times; and (4) compromise acetabular correction?
Methods
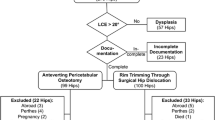
We retrospectively reviewed all 75 patients who underwent PAO for developmental dysplasia of the hip between August 2009 and May 2013. The control group included 44 consecutive patients who underwent a standard Bernese PAO with rectus takedown (RT). The study group consisted of 31 consecutive patients who underwent PAO using a modified rectus-sparing (RS) approach without routine arthrotomy. The groups were similar in age, body mass index, and American Society of Anesthesiologists score, but the RT group was comprised of a greater percentage of men than the RS group. Outcome variables were collected from patient charts and included inpatient pain, inpatient ambulation as well as length of stay, estimated blood loss, surgical time, and postoperative radiographic measurements. Cohen’s f2 was used to calculate the effect size in the regression analysis and effects were considered small for values < 0.15, moderate for 0.15 to 0.34, and large for values > 0.35.
Results
Patients who underwent PAO with a RS approach had less overall pain (RT median 4 versus RS median 2); however, the difference may not have been perceptible to the typical patient (p = 0.001, f2 = 0.059). Patients treated with the RS approach ambulated similar distances during the hospital stay with a median 11 feet (interquartile range [IQR], 0–72.5) for the RT group and a median 30 feet (IQR, 0–100) for the RS group (p = 0.215, f2 = 0.095). Patients in the RT group had a median length of stay of 4 days (IQR, 4–5) compared with a median 3 days (IQR, 3–4) in the RS group (p < 0.001). The median estimated blood loss was greater (p = 0.010) in the RT group (median, 500 mL; IQR, 350–700) versus the RS group (median, 300; IQR, 250–500). The median surgical time was longer (p < 0.001) in patients undergoing PAO with the RT approach (median, 159.5 minutes; IQR, 145.5–177) compared with the RS approach (median, 103 minutes; IQR, 75–114). Acetabular reorientation based on postoperative radiographs was not compromised by the modified approach.
Conclusions
The approach modification was straightforward to implement in all patients and did not compromise acetabular fragment mobilization or final positioning. Two of the three key variables that the approach might have influenced–pain and length of stay–were below the minimum clinically important difference and different by only a fraction of a day, respectively. The difference in ambulation was of only modest clinical importance. More definitive evidence for clinical superiority in terms of pain, ambulation, and return of muscle function will likely require more sophisticated instruments such as gait analysis, muscle strength testing, and longer-term outcome studies with sensitive instruments.
Level of Evidence
Level III, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.




Similar content being viewed by others


References
Anderson LA, Gililland J, Pelt C, Linford S, Stoddard GJ, Peters CL. Center edge angle measurement for hip preservation surgery: technique and caveats. Orthopedics. 2011;34:86.
Bernstein P, Thielemann F, Gunther KP. A modification of periacetabular osteotomy using a two-incision approach. Open Orthop J. 2007;1:13–18.
Bouttier R, Morvan J, Mazieres B, Rat AC, Ziegler LE, Fardellone P, Fautrel B, Guillemin F, Pouchot J, Roux C, Coste J, Saraux A. Reproducibility of radiographic hip measurements in adults. Joint Bone Spine. 2013;80:52–56.
Carlisle JC, Zebala LP, Shia DS, Hunt D, Morgan PM, Prather H, Wright RW, Steger-May K, Clohisy JC. Reliability of various observers in determining common radiographic parameters of adult hip structural anatomy. Iowa Orthop J. 2011;31:52–58.
Clohisy JC, Barrett SE, Gordon JE, Delgado ED, Schoenecker PL. Periacetabular osteotomy in the treatment of severe acetabular dysplasia. Surgical technique. J Bone Joint Surg Am. 2006;88(Suppl 1):65–83.
Clohisy JC, Carlisle JC, Beaule PE, Kim YJ, Trousdale RT, Sierra RJ, Leunig M, Schoenecker PL, Millis MB. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008;90(Suppl 4):47–66.
Field A. Discovering Statistics Using SPSS. London, UK: Sage Publications; 2009.
Ganz R, Klaue K, Vinh TS, Mast JW. A new periacetabular osteotomy for the treatment of hip dysplasias. Technique and preliminary results. Clin Orthop Relat Res. 1988;232:26–36.
Hussell JG, Mast JW, Mayo KA, Howie DW, Ganz R. A comparison of different surgical approaches for the periacetabular osteotomy. Clin Orthop Relat Res. 1999;363:64–72.
Mast NH, Impellizzeri F, Keller S, Leunig M. Reliability and agreement of measures used in radiographic evaluation of the adult hip. Clin Orthop Relat Res. 2011;469:188–199.
Matta JM, Stover MD, Siebenrock K. Periacetabular osteotomy through the Smith-Petersen approach. Clin Orthop Relat Res. 1999;363:21–32.
Monazzam S, Bomar JD, Cidambi K, Kruk P, Hosalkar H. Lateral center-edge angle on conventional radiography and computed tomography. Clin Orthop Relat Res. 2013;471:2233–2237.
Murphy SB, Millis MB, Hall JE. Surgical correction of acetabular dysplasia in the adult. A Boston experience. Clin Orthop Relat Res. 1999;363:38–44.
Pajarinen J, Hirvensalo E. Two-incision technique for rotational acetabular osteotomy: good outcome in 35 hips. Acta Orthop Scand. 2003;74:133–139.
Pereira F, Giles A, Wood G, Board TN. Recognition of minor adult hip dysplasia: which anatomical indices are important? Hip Int. 2014;24:175–179.
Peters CL, Erickson JA, Hines JL. Early results of the Bernese periacetabular osteotomy: the learning curve at an academic medical center. J Bone Joint Surg Am. 2006;88:1920–1926.
Selya AS, Rose JS, Dierker LC, Hedeker D, Mermelstein RJ. A practical guide to calculating Cohen’s f(2), a measure of local effect size, from PROC MIXED. Front Psychol. 2012;3:111.
Siebenrock KA, Schoeniger R, Ganz R. Anterior femoro-acetabular impingement due to acetabular retroversion. Treatment with periacetabular osteotomy. J Bone Joint Surg Am. 2003;85:278–286.
Soballe K, Troelsen A. Approaches and perioperative management in periacetabular osteotomy surgery: the minimally invasive transsartorial approach. Instr Course Lect. 2013;62:297–303.
Sucato DJ, Tulchin K, Shrader MW, DeLaRocha A, Gist T, Sheu G. Gait, hip strength and functional outcomes after a Ganz periacetabular osteotomy for adolescent hip dysplasia. J Pediatr Orthop. 2010;30:344–350.
Tan L, Aktas S, Copuroglu C, Ozcan M, Ture M. Reliability of radiological parameters measured on anteroposterior pelvis radiographs of patients with developmental dysplasia of the hip. Acta Orthop Belg. 2001;67:374–379.
Tibor LM, Sink EL. Periacetabular osteotomy for hip preservation. Orthop Clin North Am. 2012;43:343–357.
Troelsen A, Elmengaard B, Soballe K. Comparison of the minimally invasive and ilioinguinal approaches for periacetabular osteotomy: 263 single-surgeon procedures in well-defined study groups. Acta Orthop. 2008;79:777–784.
Troelsen A, Elmengaard B, Soballe K. Medium-term outcome of periacetabular osteotomy and predictors of conversion to total hip replacement. J Bone Joint Surg Am. 2009;91:2169–2179.
Trousdale RT, Cabanela ME. Lessons learned after more than 250 periacetabular osteotomies. Acta Orthop Scand. 2003;74:119–126.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
About this article

Cite this article
Peters, C.L., Erickson, J.A., Anderson, M.B. et al. Preservation of the Rectus Femoris Origin During Periacetabular Osteotomy Does Not Compromise Acetabular Reorientation. Clin Orthop Relat Res 473, 608–614 (2015). https://doi.org/10.1007/s11999-014-3837-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-014-3837-x