
Abstract
Background
Vigorous sporting activity during the growth years is associated with an increased risk of having a cam-type deformity develop. The underlying cause of this osseous deformity is unclear. One may speculate whether this is caused by reactive bone apposition in the region of the anterosuperior head-neck junction or whether sports activity alters the shape of and growth in the growth plate. If the latter is true, then one would expect athletes to show an abnormal shape of the capital growth plate (specifically, the epiphyseal extension) before and/or after physeal closure.
Questions/purposes
We therefore raised three questions: (1) Do adolescent basketball players show abnormal epiphyseal extension? (2) Does the epiphyseal extension differ before and after physeal closure? (3) Is abnormal epiphyseal extension associated with high alpha angles?
Methods
We performed a case-control comparative analysis of young (age range, 9–22 years) male elite basketball athletes with age-matched nonathletes, substratified by whether they had open or closed physes. We measured epiphyseal extension on radial-sequence MRI cuts throughout the cranial hemisphere from 9 o’clock (posterior) to 3 o’clock (anterior). Epiphyseal extension was correlated to alpha angle measurements at the same points.
Results
Epiphyseal extension was increased in all positions in the athletes compared with the control group. On average, athletes showed epiphyseal extension of 0.67 to 0.83 versus 0.53 to 0.71 in control subjects. In the control group epiphyseal extension was increased at all measurement points in hips after physeal closure compared with before physeal closure. In contrast, the subgroup of athletes with a closed growth plate only had increased epiphyseal extension at the 3 o’clock position compared with the athletes with a closed growth plate (0.64–0.70). We observed a correlation between an alpha angle greater than 55° and greater epiphyseal extension in the anterosuperior femoral head quadrant: the corresponding Spearman r values were 0.387 (all hips) and 0.285 (alpha angle > 55°) for the aggregate anterosuperior quadrant.
Conclusions
These findings suggest that a cam-type abnormality in athletes is a consequence of an alteration of the growth plate rather than reactive bone formation. High-level sports activity during growth may be a new and distinct risk factor for a cam-type deformity.
Similar content being viewed by others
Introduction
Vigorous sporting activity has been associated with the development of a cam-type deformity of the proximal femur [2, 3, 9, 12, 15, 18], although the mechanism of how this deformity arises in athletes is unknown. Murray and Duncan [12] noted an increased incidence of the tilt deformity in adolescents with compulsory sporting activity when compared with adolescents without compulsory sporting activity (24% versus 9%). Siebenrock et al. [18] reported an increased prevalence of a cam-type deformity in the anterosuperior head-neck quadrant of elite adolescent basketball players versus an age-matched control group. This alteration in head-neck contour became evident after closure of the proximal femoral physis. The resulting cam-type deformity in the anterosuperior head-neck quadrant may put the hip at risk for development of symptomatic cam-type impingement, a potential cause of early-onset osteoarthritis [5, 6, 11].
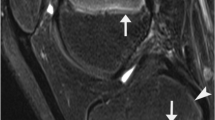
The reason for the development of a cam-type deformity in growing athletes remains unclear. One explanation could be that high stresses lead to reactive bone formation at the area of the cam-type deformity. In this case the growth plate should not be affected. However, one may speculate whether repetitive high loading forces alter physeal growth. In two studies, potential physeal changes, predominantly growth arrest, but also accelerated growth associated with chronic overload in young athletes were reported [1, 4]. Jaramillo et al. [8] described stimulation of endochondral ossification with thickening and extension of the epiphysis toward the metaphysis in experimentally induced juxtaphyseal trauma in rabbits. Theoretically, chronic overuse of the proximal femur might represent repetitive indirect trauma, which potentially could stimulate a similar growth plate extension with resultant metaphyseal deformity [8]. This is reinforced by an association between an abnormal shape of the growth plate, as measured by extension of the femoral head physis toward the neck of the femur (Fig. 1A–B), and decreased head-neck offset in adult patients with cam-type impingement [19]. A decreased head-neck offset has been inversely correlated with an increased alpha angle and is an alternative measurement for cam-type deformity [14]. Increased extension of the physeal cartilage onto the metaphysis has been associated with abnormal growth of the femoral head in Perthes disease [7]. This led to the question whether an abnormal extension of the physis onto the metaphysis also might be detected in growing athletes and whether there might be an association with a cam-type deformity.

(A) A radial-sequence MR image of the hip of a 20-year-old basketball player taken at the 2 o’clock position is shown. (B) The diameter (d) of the femoral head, through the center of the head-neck axis, and the distance from a line orthogonal to the diameter to the lateral-most extension of the epiphysis (e) is measured. The epiphyseal extension is defined as e/d. (C) The measurement of the alpha angle on this same MRI slice is shown.
We therefore asked the following questions: (1) Do adolescent basketball players show abnormal extension of the proximal femoral physis compared with age-matched control subjects? (2) Is there a change in extension of the proximal femoral physis before and after closure of the growth plate in athletes and control subjects? (3) Is abnormal extension of the proximal femoral physis associated with high alpha angles?
Patients and Methods
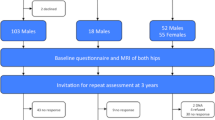
We performed a case-control study comparing a group of elite basketball athletes with a group of age-matched nonathletes (Table 1). All volunteers in both groups were included in a previous publication [18]. Volunteers had been recruited by written invitation and without reimbursement. In the previous study, we excluded patients with known hip disease, including hip dysplasia, Perthes disease, slipped capital epiphysis, or previous severe hip trauma or hip surgery. The 37 (74 hips) athletes were recruited during a 1-year period from an elite basketball club playing in the national league of Germany. The age-matched control group of 38 (76 hips) volunteers was recruited from middle, high, and medical schools in Bern, Switzerland. All volunteers were Caucasians with European nationalities. Exclusion criteria also applied in the previous study, for one (previous surgery) of the original 38 athletes and for two (too high sports level) of the original 40 less sports-active volunteers. MRI was performed on both hips in volunteers resulting in 74 MRI scans of the athletes (two MRI scans deleted for poor quality) and 76 MRI scans in the volunteer group. The age limit of 26 years in the previous study was reduced to 22 years in the current study to obtain optimal reading of the physeal scar on the MRI scans. This left 55 hip MRI scans for the athletes and 60 hip scans for the control group. Six of the original 55 MRI scans of the athletes’ hips and seven of the 60 MRI scans of the control subjects also were excluded because their physis, or physeal scar, could not be adequately seen on MRI (Table 1). Reasons for inadequate physeal observation included excessive motion artifact and normal disappearance of the physeal scar with aging. In each of the two groups, hip MRI scans were stratified into those with open physes and those with closed physes based on the radiographic appearance of the capital femoral physis on MRI (Table 1). Our hospital ethical committee approved the study and each participant gave written consent. Parent consent, in additional to personal consent, was obtained for all participants younger than 18 years.
Our key measurement variables were epiphyseal extension measured on radial-sequence MRI at each position of the cranial hemisphere from 9 o’clock (posterior femoral head-neck junction) to 3 o’clock (anterior head-neck junction) and the corresponding alpha angles (Fig. 1) [14, 19]. A proton-weighted radial sequence on a 3.0 Tesla MR system (Siemens, Erlangen, Germany) was used for evaluation of morphologic features of the proximal femur [18]. The radial planes were rotated clockwise in 30°-intervals around and perpendicular to the femoral neck axis resulting in seven hour-defined measurement points (Fig. 2). Epiphyseal extension is calculated as follows: (1) the head-neck axis is drawn through the center of the femoral head to the medial femoral head, (2) a line orthogonal to this axis is drawn starting at the medial femoral head toward the clock position being measured, (3) the distance between this line and the physeal extension is measured, parallel with the head-neck axis, and (4) this distance (e) is divided by the femoral head diameter (d) to express epiphyseal extension as a ratio (Fig. 1B). The alpha angle was measured according to the technique described by Nötzli et al. [14]. Briefly, this is the angle between the femoral neck axis and a line connecting the femoral head center with a point, where the femoral head contours leaves a best-fit circle around it (Fig. 1C, Fig. 2).

(A) Radial-sequence MRI planes are perpendicular to the femoral head-neck axis. (B) Positions are defined clockwise with the 12 o’clock position being superior and 3 o’clock position being anterior; 3 h = 3 hours; 6 h = 6 hours; 9 h = 9 hours; 12 h = 12 hours. (Published with permission from Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC. The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res. 2011;469:3229–3240.)
Based on a previous study by Siebenrock et al. [19] of epiphyseal extension in patients versus healthy control subjects, we performed a power analysis. We calculated study power to detect a difference in means of 0.13 with a measurement SD of 0.10 for epiphyseal extension. These criteria represent substantial visible changes in epiphyseal extension and were chosen to ensure adequate sample size was available for this study. A minimum of 18 patients in each group would yield a power of 96.6% at a two-sided p of 0.05.
Normal distribution of our key measurement variables was determined with the Kolmogorov-Smirnov test. We determined differences between the groups for alpha angles and epiphyseal extension using Student’s t-test. For correlating values of the epiphyseal extension and the alpha angle at each corresponding measurement point, we used the Spearman rank correlation test. All statistical analyses were performed using R version 2.14.1 (R Foundation for Statistical Computing, Vienna, Austria) [16].
Results
Athletes had greater epiphyseal extension than control subjects (p < 0.001) at all positions (Fig. 3). Epiphyseal extension was greatest posterosuperiorly in all subgroups (Table 2). When comparing subgroups, there was a marked increase in epiphyseal extension in athletes with open physes compared with control subjects (Fig. 4A). After physeal closure, epiphyseal extension remained greater in athletes compared with control subjects; however, the difference between the two groups was reduced (Fig. 4B).

Epiphyseal extension for all athletes and all control subjects is shown for the cranial half of the femoral head-neck junction (9 o’clock through 3 o’clock). Epiphyseal extension is greater in athletes than control subjects for all positions (p < 0.001).

Epiphyseal extension for athletes and control subjects is shown for (A) open and (B) closed physes. Although there is a marked difference between the two groups when the physis is open, the difference narrows after physeal closure.
In athletes, the subgroup with a closed physis showed a lower epiphyseal extension at the 11 (0.844–0.810; p = 0.016) and 12 o’clock (0.820–0.785; p = 0.041) positions and increased extension (0.641–0.701; p < 0.005) at the 3 o’clock position (Fig. 5A) compared with the subgroup with an open physis. In the control group, epiphyseal extension was greater at all positions (p < 0.01 at all positions) in the subgroup with a closed physis compared with the subgroup with an open physis (Fig. 5B).

A comparison is shown between epiphyseal extension before and after physeal closure for (A) athletes and (B) control subjects. Athletes with open physes show epiphyseal extensions in the range of their counterparts with closed physes. Control subjects show a relatively uniform increase in epiphyseal extension as the growth plate closes.
The mean alpha angles at each clockwise measurement point are shown (Table 3). When evaluating all 102 hips, a positive correlation between an increased epiphyseal extension and a high alpha angle was seen at the 1 o`clock and 3 o`clock positions. The corresponding Spearman correlation coefficient r values were 0.215 (p = 0.031) at the 1 o’clock position and 0.352 (p < 0.001) at the 3 o’clock position (Table 4). When evaluating hips with alpha angles greater than 55°, the Spearman correlation coefficient r values were 0.322 (p = 0.038; n = 15) at the 1 o’clock position and 0.715 (p < 0.009; n = 12) at the 3 o’clock position. Finally, when evaluating the relationship between alpha angle and epiphyseal extension of the anterosuperior quadrant in aggregate, the Spearman correlation coefficient r values were 0.387 (p < 0.001; n = 102) in all hips and 0.285 (p < 0.006; n = 92) in hips with alpha angles greater than 55° (Fig. 6).

A scatterplot with linear regression line shows the relationship between the alpha angle and epiphyseal extension in the anterosuperior quadrant of all hips (1 o’clock through 3 o’clock positions).
Discussion
High-level sports activity during the growth years is associated with an increased risk for development of a cam-type deformity [2, 3, 9, 12, 15, 18]. One may speculate whether this is caused by reactive bone apposition at the anterosuperior head-neck junction or whether sports activity alters the shape of the growth plate. If the latter is true, then one would expect athletes to show an abnormal shape of the capital growth plate (specifically, the epiphyseal extension) before and/or after physeal closure. We therefore asked the following questions: (1) Do adolescent basketball players show abnormal extension of the proximal femoral physis compared with age-matched control subjects? (2) Is there a difference in epiphyseal extension before and after closure of the growth plate in athletes and control subjects? (3) Is abnormal extension of the proximal femoral physis associated with high alpha angles?
There are several limitations to this study. First, although we detected an altered physeal shape in athletes, the ultimate impact on morphologic features of the proximal femur and subsequent joint function remains unclear. Our retrospective, descriptive design allows us to determine only morphologic associations and does not allow us to describe the underlying mechanisms for the observed physeal alterations. Although a correlation between alpha angles greater than 55° and greater physeal extension could be detected, it remains unclear whether these findings will lead to a symptomatic cam-type impingement with pain and cartilage lesions. However this was beyond the scope of the study. The athletes were active on an elite level and none of the included individuals was considered for treatment of hip impingement so far.
Accelerated and excessive physeal extension in basketball players might be triggered by athletic activities. The fact that greater physeal extension is visible and most pronounced in a young age group (range, 9.3–16.2 years) with an open physis suggests an early mechanism interfering with growth. Because increased alpha angles in the same athlete group became visible typically after closure of the growth plate [18], increased physeal extension seems to be an initial event that precedes the cam-type deformity. One may speculate whether accelerated growth with chronic overload in the throwing shoulder of adolescent baseball pitchers follows a similar pattern [1]. Another example is the altered and extended cartilage extension onto the metaphysis as seen on plain radiographs preceding head deformity in Perthes disease [7].
Epiphyseal extension in the control subjects uniformly was greater in the subgroup with a closed physis versus the subgroup with an open physis. In the athletes there was a nonuniform pattern of change when hips with an open physis were compared with hips with a closed physis (Table 2; Fig. 5). A decrease in the epiphyseal extension was seen in athletes in the posterosuperior quadrant after physeal closure, while we measured an increase in the anterosuperior quadrant (Fig. 5A). One may speculate whether this pattern represents irregular growth velocity or early focal physeal closure. Early physeal arrest has been described predominantly in the upper extremities of overhead throwing athletes [13, 17].
The epiphyseal extension in our control group is consistent with data from a recently published longitudinal study in school children [10]. Increased physeal extension was observed in the upper half of the femoral head before growth plate closure in children [10]. When divided through head size, Kienle et al. [10] measured ranges of epiphyseal extension from 50% to 71% in hips with open physes (49%–69% in our study) and 56% to 74% in hips with closed physes (60%–75% in our study) (Table 5). In addition, the pattern of physeal extension was similar, with the highest values measured in the posterosuperior quadrant. Siebenrock et al. [19] reported epiphyseal extensions ranging from 67% to 88% in adult probands with a higher mean age of 26.3 years. Because the physeal scar fades with time, it becomes increasingly more difficult to trace the physeal line, perhaps leading to the higher values reported in that older group [19]. In addition, it is unknown how the appearance of the physeal scar might change during a lifetime and more data for comparison of older age groups are needed.
We present some evidence to suggest epiphyseal extension correlates with alpha angles (Table 4; Fig. 6). When evaluating all hips, the epiphyseal extension correlated with the alpha angle at the 1 o’clock and 3 o’clock positions. Furthermore, the correlation at these positions strengthened when limiting the evaluation to patients with alpha angles greater than 55°. When evaluating the anterosuperior quadrant in aggregate, the correlation remained. This would indicate abnormally high alpha angles in the anterosuperior head-neck junction were associated with increased epiphyseal extension. These findings are consistent with previously published data in which greater epiphyseal extension correlated with decreased head-neck offset (ie, suggesting cam-type deformity) in the anterosuperior quadrant in patients treated for symptomatic cam-type impingement [19]. One may assume the number and degree of cam-type deformities in our athletes were too low to provide meaningful statistics regarding symptomatic cam-type femoroacetabular impingement. However the data suggest a link between athletic activity during growth and the formation of a cam-type deformity as measured by increased alpha angles in the typical location, the anterosuperior quadrant of the femoral head. This would agree with Murray and Duncan [12], who speculated that a more than threefold increase of a tilt deformity of the proximal femur in athletes might be triggered by vigorous sporting activity during adolescence.
Young basketball athletes had larger extension of the capital growth plate toward the neck throughout the entire cranial hemisphere. This finding already was visible and most pronounced during growth before physeal closure. A correlation between increased extension of the growth plate in the anterosuperior quadrant and increased alpha angles suggests a causal link, but more study is needed. Thus, an altered shape of the growth plate may precede a cam-type deformity in basketball athletes suggesting a developmental abnormality. It is unclear whether or how many athletes with this developmental cam-type deformity will progress to symptomatic cam-type femoroacetabular impingement.
References
Adams JE. Little league shoulder: osteochondrosis of the proximal humeral epiphysis in boy baseball pitchers. Calif Med. 1966;105:22–25.
Bharam S. Labral tears, extra-articular injuries, and hip arthroscopy in the athlete. Clin Sports Med. 2006;25:279–292, ix.
Bizzini M, Nötzli HP, Maffiuletti NA. Femoroacetabular impingement in professional ice hockey players: a case series of 5 athletes after open surgical decompression of the hip. Am J Sports Med. 2007;35:1955–1959.
Caine D, DiFiori J, Maffulli N. Physeal injuries in children’s and youth sports: reasons for concern? Br J Sports Med. 2006;40:749–760.
Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: an integrated mechanical concept. Clin Orthop Relat Res. 2008;466:264–272.
Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120.
Jaramillo D, Kasser JR, Villegas-Medina OL, Gaary E, Zurakowski D. Cartilaginous abnormalities and growth disturbances in Legg-Calvé-Perthes disease: evaluation with MR imaging. Radiology. 1995;197:767–773.
Jaramillo D, Laor T, Zaleske DJ. Indirect trauma to the growth plate: results of MR imaging after epiphyseal and metaphyseal injury in rabbits. Radiology. 1993;187:171–178.
Keogh MJ, Batt ME. A review of femoroacetabular impingement in athletes. Sports Med. 2008;38:863–878.
Kienle KP, Keck J, Werlen S, Kim YJ, Siebenrock KA, Mamisch TC. Femoral morphology and epiphyseal growth plate changes of the hip during maturation: MR assessments in a 1-year follow-up on a cross-sectional asymptomatic cohort in the age range of 9-17 years. Skeletal Radiol. 2012;41:1381–1390.
Leunig M, Beaulé PE, Ganz R. The concept of femoroacetabular impingement: current status and future perspectives. Clin Orthop Relat Res. 2009;467:616–622.
Murray RO, Duncan C. Athletic activity in adolescence as an etiological factor in degenerative hip disease. J Bone Joint Surg Br. 1971;53:406–419.
Nanni M, Butt S, Mansour R, Muthukumar T, Cassar-Pullicino VN, Roberts A. Stress-induced Salter-Harris I growth plate injury of the proximal tibia: first report. Skeletal Radiol. 2005;34:405–410.
Nötzli H, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002;84:556–560.
Philippon M, Schenker M, Briggs K, Kuppersmith D. Femoroacetabular impingement in 45 professional athletes: associated pathologies and return to sport following arthroscopic decompression. Knee Surg Sports Traumatol Arthrosc. 2007;15:908–914.
R Development Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria; 2011. Available at: http://www.R-project.org/. Accessed August 21, 2012.
Sato T, Shinozaki T, Fukuda T, Watanabe H, Aoki J, Yanagawa T, Takagishi K. Atypical growth plate closure: a possible chronic Salter and Harris Type V injury. J Pediatr Orthop B. 2002;11:155–158.
Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC. The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res. 2011;469:3229–3240.
Siebenrock KA, Wahab KH, Werlen S, Kalhor M, Leunig M, Ganz R. Abnormal extension of the femoral head epiphysis as a cause of cam impingement. Clin Orthop Relat Res. 2004;418:54–60.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (JMS) has received fellowship funding from the Maurice E. Müller Foundation of North America. Each author certifies that he or she, or a member of his or her immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Siebenrock, K.A., Behning, A., Mamisch, T.C. et al. Growth Plate Alteration Precedes Cam-type Deformity in Elite Basketball Players. Clin Orthop Relat Res 471, 1084–1091 (2013). https://doi.org/10.1007/s11999-012-2740-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2740-6