
Abstract
Purpose of Review
While we started clinical trials evaluating the benefit of lowering systolic BP’s >160 mm Hg and diastolic BPs of <130 mm Hg, the latest guideline suggests a target of <130/80 mm Hg in those with hypertension. This article summarizes exactly how we got to where we are looking over the last half-century.
Recent Findings
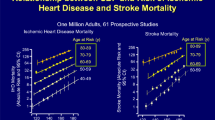
Our understanding of systolic and diastolic blood pressure targets to improve cardiovascular outcomes has changed substantially over the past 5 decades. Regarding diastolic blood pressure targets to improve cardiovascular outcomes, initially the VA1 in 1967 had set the goal to <115 mmHg. Over time, several studies including the VA2, Hypertension Optimal Treatment (HOT), and United Kingdom Prospective Diabetes Study Group 38 (UKPDS38) highlighted even greater cardiovascular benefit with lower diastolic targets <80 mmHg, especially in diabetic patients. Of equal importance, multiple studies have focused the attention to systolic blood pressure targets. Starting in 1948 with the Framingham study, passing through the Systolic Hypertension in the Elderly Program (SHEP), Syst-Eur and Syst-China trials, all have set the systolic blood pressure goal <150 mmHg. Most recently, the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial showed an improved cardiovascular outcome with a systolic blood pressure target <140 mmHg in patients with type 2 diabetes, while the Systolic Blood Pressure Intervention Trial (SPRINT) in non-diabetic patients moved it closer to 120 mmHg.
Summary
There is “no one size fits all” when it comes to blood pressure targets to improve cardiovascular outcomes. To progress our understanding of individual blood pressure goals, future studies might develop a more standardized approach to highlight characteristics such as design and end point definitions while allowing clinical practitioners greater latitude to adapt guideline recommendations to individual patient characteristics and clinical needs.



Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289(19):2560–72.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–20.
Hoots WK, Kiley JP, Mockrin SC, Lauer M, Mensah GA, Patel Y, et al. NHLBI strategic visioning: setting an agenda together for the NHLBI of 2025. Blood. 2015;125(17):2733–5.
Nerenberg KA, Zarnke KB, Leung AA, Dasgupta K, Butalia S, McBrien K, et al. Hypertension Canada’s 2018 guidelines for diagnosis, risk assessment, prevention, and treatment of hypertension in adults and children. Can J Cardiol. 2018;34(5):506–25.
•• Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ ACPM/AGS/APhA/ ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Soc Hypertens. 2018;12(8):579.e571–3 Current guidelines recommend a target SBP <130 mmHg for all hypertensive patients, including the elderly.
Welch NA. Medical aspects of hypertension. N Engl J Med. 1946;235(21):752–4.
Ha SK. Dietary salt intake and hypertension. Electrolyte Blood Press. 2014;12(1):7–18.
Smithwick RH. Hypertensive cardiovascular disease; effect of thoracolumbar splanchnicectomy on mortality and survival rates. J Am Med Assoc. 1951;147(17):1611–5.
•• Effects of treatment on morbidity in hypertension. Results in patients with diastolic blood pressures averaging 115 through 129 mm Hg. JAMA. 1967;202(11):1028–34 VA1 lowered the general DBP target to <115 mmHg.
•• Kannel WB, Gordon T, Schwartz MJ. Systolic versus diastolic blood pressure and risk of coronary heart disease. The Framingham study. Am J Cardiol. 1971;27(4):335–46 The study shifted the attention to include SBP targets and older populations in interventional trials.
Effects of treatment on morbidity in hypertension. II. Results in patients with diastolic blood pressure averaging 90 through 114 mm Hg. JAMA. 1970;213(7):1143–52.
• Hansson L, Zanchetti A, Carruthers SG, et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet. 1998;351(9118):1755–62 The study supported the cardiovascular benefit of DBP target of ≤80 mmHg and supported a SBP target of <150 mmHg.
• Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317(7160):703–13 The study supported a DBP target of ≤85 mmHg.
• Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358(18):1887–98 The study concluded that a DBP <80mmHg (and SBP <150 mmHg) in the very elderly >80 years old was safe, reduced total mortality, and effectively reduced the risks of the cardiovascular outcomes studied.
Bulpitt CJ, Beckett NS, Cooke J, Dumitrascu DL, Gil-Extremera B, Nachev C, et al. Results of the pilot study for the Hypertension in the Very Elderly Trial. J Hypertens. 2003;21(12):2409–17.
Society of Actuaries. Build and Blood Pressure Study. Chicago: The Society. 1959;1:268.
Stamler J. Lectures on preventive cardiology. New York: Grune & Stratton; 1967.
Shekelle ROA, KJawans H. Hypertension and risk of stroke in an elderly population. Stroke. 1974;5:71–5.
•• Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research Group. JAMA. 1991;265(24):3255–64 The study showed the cardiovascular benefits of lowering SBP targets in those with ISH to <150 mmHg.
• Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 1997;350(9080):757–64 The study confirmed the cardiovascular benefits of ISH target of <150 mmHg in non-US population, previously shown in SHEP trial.
• Wang JG, Staessen JA, Gong L, Liu L. Chinese trial on isolated systolic hypertension in the elderly. Systolic Hypertension in China (Syst-China) Collaborative Group. Arch Intern Med. 2000;160(2):211–20 The study confirmed the cardiovascular benefit of SBP target of <150 mmHg in non-US population with ISH, previously shown in Syst-Eur and SHEP trials.
•• Buse JB, Bigger JT, Byington RP, et al. Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial: design and methods. Am J Cardiol. 2007;99(12a):21i–33i The study showed a beneficial cardiovascular effect of a lower SBP target of <140 mmHg in AODM2.
Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281–357.
•• Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103–16 The study moved the SBP target closer to 120 mmHg.
• Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–104.
Kim KI, Ihm SH, Kim GH, Kim HC, Kim JH, Lee HY, et al. 2018 Korean society of hypertension guidelines for the management of hypertension: part III-hypertension in special situations. Clin Hypertens. 2019;25:19.
Acknowledgements
Drs. Herbeth, Fülöp and Basile are current employee of the United States Department of Veteran Health Administrations. However, the views and opinions expressed herewith do not reflect the official views or opinion or endorsed by the United States Veteran Health Administrations.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Conflict of Interest
The authors declare no conflicts of interest relevant to this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Guidelines / Clinical Trials/Meta-Analysis
Rights and permissions
About this article

Cite this article
Herberth, J., Soliman, K.M., Fülöp, T. et al. How We Got Where We Are in Blood Pressure Targets. Curr Hypertens Rep 23, 33 (2021). https://doi.org/10.1007/s11906-021-01143-8
Accepted:
Published:
DOI: https://doi.org/10.1007/s11906-021-01143-8