Abstract
Objective
The preferred surgical approach for systemic-pulmonary shunts has changed from thoracotomy to sternotomy in our institution, to concomitantly manage the ductus arteriosus during surgery. The purpose of this study was to compare the outcomes of systemic-pulmonary shunts for neonates with functionally univentricular hearts based on surgical approach.
Methods
Fifty-two neonates with functionally univentricular hearts underwent systemic-pulmonary shunt via sternotomy (n = 28) or thoracotomy (n = 24). Patient characteristics, achievement rates of right heart bypass, and survival rates were compared for the different approaches.
Results
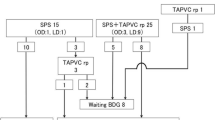
Prenatal diagnosis was made more common in the sternotomy group (p = 0.006). The shunt was placed more centrally in the sternotomy group. The ductus arteriosus was ligated or banded in most patients in the sternotomy group (26/28) and in a few patients in the thoracotomy group (6/24). Frequency of ductal management in the early postoperative phase was not different between the groups (21 vs 25 %), but three new incisions had to be made in the thoracotomy group. No differences were seen in the achievement rates of bidirectional cavopulmonary shunts (86 vs 87 % at 10 months of age) and total cavopulmonary connection (81 vs 81 % at 2 years of age), or in the survival rates (92 vs 96 % at 8 years).
Conclusions
There were no differences in short- and long-term outcomes between the groups. The sternotomy approach might be preferable in the current era of prenatal diagnosis, to allow simultaneous duct management during systemic-pulmonary shunt surgery, particularly in patients with large ducts associated with functionally univentricular hearts.





Similar content being viewed by others

References
Kouchoukos NT, Blackstone EH, Doty DB, Hanley FL, Karp RB. Cardiac surgery, 3rd edn. Chapter 27 Tricuspid atresia and management of single-ventricle physiology, pp. 1113–1175.
Talwar S, Kumar MV, Muthukkumaran S, Airan B. Is sternotomy superior to thoracotomy for modified Blalock–Taussig shunt? Interact CardioVasc Thorac Surg. 2014;18(3):371–5.
Kajihara N, Asou T, Takeda Y, Kosaka Y, Miyata D, Nagafuchi H, Yasui S. Impact of 3-mm Blalock–Taussig shunt in neonates and infants with a functionally single ventricle. Interact CardioVasc Thorac Surg. 2009;8:211–5.
Quartermain MD, Pasquali SK, Hill KD, Goldberg DJ, Huhta JC, Jacobs JP, Jacobs ML, Kim S, Ungerleider RM. Variation in prenatal diagnosis of congenital heart disease in infants. Pediatrics. 2015;136:e378–85.
Zahorec M, Hrubsova Z, Skrak P, Poruban R, Nosal M, Kovacikova L. A comparison of Blalock–Taussig shunts with and without closure of the ductus arteriosus in neonates with pulmonary atresia. Ann Thorac Surg. 2011;92:653–9.
Petrucci O, O’Brien SM, Jacobs ML, Jacobs JP, Manning PB, Eghtesady P. Risk factors for mortality and morbidity after the neonatal Blalock–Taussig shunt procedure. Ann Thorac Surg. 2011;92:642–52.
Alsoufi B, Gillespie S, Kogon B, Schlosser B, Sachdeva R, Kim D, Clabby M, Kanter K. Results of palliation with an initial modified Blalock–Taussig shunt in neonates with single ventricle anomalies associated with restrictive pulmonary blood flow. Ann Thorac Surg. 2015;99:1639–47.
O’Connor MJ, Ravishankar C, Ballweg JA, Gillespie MJ, Gaynor JW, Tabbutt S, Dominguez TE. Early systemic-to-pulmonary artery shunt intervention in neonates with congenital heart disease. J Thorac Cardiovasc Surg. 2011;142:106–12.
Ichikawa Y, Yokoyama U, Iwamoto M, Oshikawa J, Okumura S, Sato M, Yokota S, Masuda M, Asou T, Ishikawa Y. Inhibition of phosphodiesterase type 3 dilates the rat ductus arteriosus without inducing intimal thickening. Circ J. 2012;76(10):2456–64.
Smith GC. The pharmacology of the ductus arteriosus. Pharmacol Rev. 1998;50(1):35–58.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Rights and permissions
About this article

Cite this article
Sasaki, T., Takeda, Y., Ohnakatomi, Y. et al. Surgical approach for systemic-pulmonary shunt in neonates with functionally univentricular heart: comparison between sternotomy and thoracotomy. Gen Thorac Cardiovasc Surg 64, 529–536 (2016). https://doi.org/10.1007/s11748-016-0673-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-016-0673-9