
Abstract
Background
Significant weight-loss and diabetes remission have been reported after mini-gastric bypass (MGB). Concern has been raised regarding postoperative bile reflux (BR), but it has not been demonstrated in previous studies. We set out to find out if BR is evident in hepatobiliary scintigraphy after MGB.
Methods
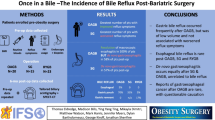
Nine consecutive patients, seven with type 2 diabetes, underwent MGB (15 cm gastric tube, 250–275 cm biliary limb) at our institution with a 12-month follow-up, with none lost to follow-up. Then, 10.7 months (8.6–13.0) after MGB, all patients underwent hepatobiliary scintigraphy and a reflux symptom questionnaire (GerdQ) was filled out. A gastroscopy with biopsies was done for all patients with a bile-reflux-positive scintigraphy.
Results
Mean age at operation was 56 years (41–65) and preoperative BMI 43.1 kg/m2 (34.2–54.6). Mean %EWL was 83.9 (49.5–128.3) at 12 months. Four patients reached diabetes remission and two became insulin-independent. Hepatobiliary scintigraphy showed a transient BR into the gastric tube for five patients. Bile tracer was found in the gastric tube at 23–58 min after the tracer injection and highest activity was 8% (1–8%) at 58 min. Bile tracer was not found in the esophagus of any of the patients. One patient with a positive scintigraphy in the gastric tube required re-operation. Two patients with reflux symptoms had a negative scintigraphy.
Conclusion
Our results indicate that transient bile reflux is common after MGB in the gastric tube, but not in the esophagus. The clinical relevance of bile reflux needs further studies.


Similar content being viewed by others


References
Rutledge R. The mini-gastric bypass: experience with the first 1,274 cases. Obesity Surg. 2001;11(3):276–80.
Noun R, Skaff J, Riachi E, et al. One thousand consecutive mini-gastric bypass: short- and long-term outcome. Obesity Surg. 2012;22(5):697–703.
Lee W, Yu P, Wang W, et al. Laparoscopic Roux-en-Y versus mini-gastric bypass for the treatment of morbid obesity: a prospective randomized controlled clinical trial. Ann Surg. 2005;242(1):20–8.
Lee WJ, Ser KH, Lee YC, et al. Laparoscopic Roux-en-Y vs. mini-gastric bypass for the treatment of morbid obesity: a 10-year experience. Obesity Surg. 2012;22(12):1827–34.
Victorzon M. Single-anastomosis gastric bypass: better, faster, and safer? Scand J Surg. 2015;104(1):48–53.
Johnson WH, Fernanadez AZ, Farrell TM, et al. Surgical revision of loop ("mini") gastric bypass procedure: multicenter review of complications and conversions to Roux-en-Y gastric bypass. Surgery for Obesity & Related Diseases. 2007;3(1):37–41.
Stein HJ, Smyrk TC, DeMeester TR, et al. Clinical value of endoscopy and histology in the diagnosis of duodenogastric reflux disease. Surgery. 1992; discussion 803-4112(4):796–803.
Mittal BR, Ibrarullah M, Agarwal DK, et al. Comparative evaluation of scintigraphy and upper gastrointestinal tract endoscopy for detection of duodenogastric reflux. Ann Nucl Med. 1994;8(3):183–6.
Chen TF, Yadav PK, Wu RJ, et al. Comparative evaluation of intragastric bile acids and hepatobiliary scintigraphy in the diagnosis of duodenogastric reflux. World J Gastroenterol. 2013;19(14):2187–96.
Yumuk V, Tsigos C, Fried M, et al. European guidelines for obesity management in adults. Obesity Facts. 2015;8(6):402–24.
Jones R, Junghard O, Dent J, et al. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Aliment Pharmacol Ther. 2009;30(10):1030–8.
Tulchinsky M, Ciak BW, Delbeke D, et al. SNM practice guideline for hepatobiliary scintigraphy 4.0. J Nucl Med Technol. 2010;38(4):210–8.
McCarthy HB, Rucker RDJ, Chan EK, et al. Gastritis after gastric bypass surgery. Surgery. 1985;98(1):68–71.
Chevallier JM, Arman GA, Guenzi M, et al. One thousand single anastomosis (omega loop) gastric bypasses to treat morbid obesity in a 7-year period: outcomes show few complications and good efficacy. Obesity Surg. 2015;25(6):951–8.
Iftikhar SY, Ledingham S, Steele RJ, et al. Bile reflux in columnar-lined Barrett's oesophagus. Ann R Coll Surg Engl. 1993;75(6):411–6.
Martinez de Haro L, Ortiz A, Parrilla P, et al. Intestinal metaplasia in patients with columnar lined esophagus is associated with high levels of duodenogastroesophageal reflux. Ann Surg. 2001;233(1):34–8.
Dixon MF, Mapstone NP, Neville PM, et al. Bile reflux gastritis and intestinal metaplasia at the cardia. Gut. 2002;51(3):351–5.
Nason KS, Farrow DC, Haigh G, et al. Gastric fluid bile concentrations and risk of Barrett's esophagus. Interactive Cardiovascular & Thoracic Surgery. 2007;6(3):304–7.
Li XB, Lu H, Chen HM, et al. Role of bile reflux and Helicobacter pylori infection on inflammation of gastric remnant after distal gastrectomy. J Dig Dis. 2008;9(4):208–12.
Chen S, Mo J, Cao Z, et al. Effects of bile reflux on gastric mucosal lesions in patients with dyspepsia or chronic gastritis. World J Gastroenterol. 2005;11(18):2834–7.
Dixon MF, Neville PM, Mapstone NP, et al. Bile reflux gastritis and Barrett's oesophagus: further evidence of a role for duodenogastro-oesophageal reflux? Gut. 2001;49(3):359–63.
McQuaid KR, Laine L, Fennerty MB, et al. Systematic review: the role of bile acids in the pathogenesis of gastro-oesophageal reflux disease and related neoplasia. Aliment Pharmacol Ther. 2011;34(2):146–65.
Park MJ, Kim KH, Kim HY, et al. Bile acid induces expression of COX-2 through the homeodomain transcription factor CDX1 and orphan nuclear receptor SHP in human gastric cancer cells. Carcinogenesis. 2008;29(12):2385–93.
Tolin RD, Malmud LS, Stelzer F, et al. Enterogastric reflux in normal subjects and patients with Bilroth II gastroenterostomy. Measurement of enterogastric reflux. Gastroenterology. 1979;77(5):1027–33.
Mackie C, Hulks G, Cuschieri A. Enterogastric reflux and gastric clearance of refluxate in normal subjects and in patients with and without bile vomiting following peptic ulcer surgery. Ann Surg. 1986;204(5):537–42.
Tolone S, Cristiano S, Savarino E, et al. Effects of omega-loop bypass on esophagogastric junction function. Surg Obes Relat Dis. 2016;12(1):62–9.
Mahawar KK, Carr WR, Balupuri S, et al. Controversy surrounding 'mini' gastric bypass. Obes Surg. 2014;24(2):324–33.
Sundbom M, Hedenstrom H, Gustavsson S. Duodenogastric bile reflux after gastric bypass: a cholescintigraphic study. Digestive Diseases & Sciences. 2002;47(8):1891–6.
Schafer LW, Larson DE. Melton LJ3, Higgins JA, Ilstrup DM. The risk of gastric carcinoma after surgical treatment for benign ulcer disease. A population-based study in Olmsted County, Minnesota. N Engl J Med. 1983;309(20):1210–3.
Viste A, Bjornestad E, Opheim P, et al. Risk of carcinoma following gastric operations for benign disease. A historical cohort study of 3470 patients. Lancet. 1986;2(8505):502–5.
Scozzari G, Trapani R, Toppino M, et al. Esophagogastric cancer after bariatric surgery: systematic review of the literature. Surgery for Obesity & Related Diseases. 2013;9(1):133–42.
Wu C, Lee W, Ser K, et al. Gastric cancer after mini-gastric bypass surgery: a case report and literature review. Asian Journal of Endoscopic Surgery. 2013;6(4):303–6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Ethical Approval
This study was approved by the surgical ethics committee of our institution.
Sources of Funding
This study was funded by Finnish governmental research funds (EVO).
Rights and permissions
About this article

Cite this article
Saarinen, T., Räsänen, J., Salo, J. et al. Bile Reflux Scintigraphy After Mini-Gastric Bypass. OBES SURG 27, 2083–2089 (2017). https://doi.org/10.1007/s11695-017-2608-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-2608-7