
Abstract
Background
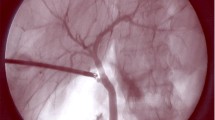
Fluorescence cholangiography represents an incisionless technique that can be applied during laparoscopic cholecystectomy to visualize bile ducts. Our objective was to evaluate and detect variances of fluorescence imaging in obese and non-obese patients.
Methods
Prospective patients were selected for laparoscopic cholecystectomies. Subjects were divided into groups based on their body mass index. Fluorescence imaging was applied preceding any dissection of extrahepatic ducts and again after dissection. Positive and negative identifications of biliary ducts were recorded.
Results
Seventy-one patients participated, with 53.5 % classified as obese. The cystic, hepatic, common bile duct, and accessory ducts were identified as follows: 100, 70.4, 87.3, and 7.0 % of patients, respectively. No differences in hepatic duct, common bile duct, and accessory duct visualization were detected in the obese and non-obese groups (p value 0.09, 0.16, and 0.66, respectively).
Conclusions
Fluorescent cholangiography is a useful technique in the obese and non-obese population. Obesity does not affect fluorescence visualization of bile ducts.



Similar content being viewed by others


References
Buddingh KT, Nieuwenhuijs VB, van Buuren L, et al. Intraoperative assessment of biliary anatomy for prevention of bile duct injury: a review of current and future patient safety interventions. Surg Endosc. 2011;25:2449–61.
Olsen D. Bile duct injuries during laparoscopic cholecystectomy. Surg Endosc. 1997;11:133–8.
Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180:101–25.
Lam T, Usatoff V, Chan ST. Are we getting the critical view? A prospective study of photographic documentation during laparoscopic cholecystectomy. HPB (Oxford). 2014;16:859–63.
Hakamada K, Narumi S, Toyoki Y, et al. Intraoperative ultrasound as an educational guide for laparoscopic biliary surgery. World J Gastroenterol. 2008;14(15):2370–6.
Berci G, Hunter J, Morgenstern L, et al. Laparoscopic cholecystectomy: first, do no harm; second, take care of bile duct stones. Surg Endosc. 2013;27:1051–4.
Way LW, Stewart L, Gantert W, et al. Causes and prevention of laparoscopic bile duct injuries: analysis of 252 cases from a human factors and cognitive psychology perspective. Ann Surg. 2003;237:460–9.
Spinoglio G, Priora F, Bianchi PP, et al. Real-time near-infrared (NIR) fluorescent cholangiography in single-site robotic cholecystectomy (SSRC): a single-institutional prospective study. Surg Endosc. 2013;27:2156–62.
Ishizawa T, Bandai Y, Ijichi M, et al. Fluorescent cholangiography illuminating the biliary tree during laparoscopic cholecystectomy. Br J Surg. 2010;97:1369–77.
Schols RM, Lodewick TM, Bouvy ND, et al. Near-infrared fluorescence laparoscopy of the cystic duct and artery in pigs: performance of a preclinical dye. J Laparoendosc Adv Surg Tech A. 2014;24:318–22.
Dip FD, Nahmod M, Anzorena FS, et al. Novel technique for identification of ureters using sodium fluorescein. Surg Endosc. 2014;28:2730–3.
Dip FD, Roy M, Perrins S, et al. Technical description and feasibility of laparoscopic adrenal contouring using fluorescence imaging. Surg Endosc. 2015;29(3):569–74.
Kaneko J, Ishizawa T, Masuda K, et al. Indocyanine green reinjection technique for use in fluorescent angiography concomitant with cholangiography during laparoscopic cholecystectomy. Surg Laparosc Endosc Percutan Tech. 2012;22:341–4.
Dip FD, Asbun D, Rosales-Velderrain A, et al. Cost analysis and effectiveness comparing the routine use of intraoperative fluorescent cholangiography with fluoroscopic cholangiogram in patients undergoing laparoscopic cholecystectomy. Surg Endosc. 2014;28:1838–43.
Ishizawa T, Kaneko J, Inoue Y, et al. Application of fluorescent cholangiography to single-incision laparoscopic cholecystectomy. Surg Endosc. 2011;25:2631–6.
Osayi S, Wendling M, Drosdeck J, et al. Near-infrared fluorescent cholangiography facilitates identification of biliary anatomy during laparoscopic cholecystectomy. New York: Springer Science Business Media; 2014.
R Core Team (2013). R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/Documento3.
Suman Kundu, Yurii S. Aulchenko, A. Cecile J.W. Janssens (2012). PredictABEL: Assessment of risk prediction models. R package version 1.2-1. http://CRAN.R-project.org/package=PredictABEL.
Hosmer DW, Lemeshow S. Applied logistic regression. New York: Wiley; 2000.
Daskalaki D, Fernandes E, Wang E. Indocyanine green (ICG) fluorescent cholangiography during robotic cholecystectomy: results of 184 consecutive cases in a single institution. Surg Innov. 2014;21(6):615–21.
Mitsuhashi N, Kimura F, Shimizu H, et al. J Hepatobiliary Pancreat Surg. 2008;15:508–14.
Verbeek FP, Schaafsma BE, Tummers QR, et al. Optimization of near-infrared fluorescence cholangiography for open and laparoscopic surgery. Surg Endosc. 2014;28:1076–82.
Buchs NC, Pugin F, Azagury DE, et al. Real-time near-infrared fluorescent cholangiography could shorten operative time during robotic single-site cholecystectomy. Surg Endosc. 2013;27:3897–901.
Ishizawa T, Bandai Y, Kokudo N. Fluorescent cholangiography using indocyanine green for laparoscopic cholecystectomy: an initial experience. Arch Surg. 2009;144:381–2.
Alander JT, Kaartinen I, Laakso A, et al. A review of indocyanine green fluorescent imaging in surgery. Int J Biomed Imaging. 2012;2012:940585.
Kim JH, Kim WH, Kim JH, et al. Management of patients who return to the hospital with a bile leak after laparoscopic cholecystectomy. J Laparoendosc Adv Surg Tech A. 2010;20:317–22.
Balija M, Huis M, Szerda F, et al. Laparoscopic cholecystectomy—accessory bile ducts. Acta Med Croatica. 2003;57:105–9.
Scroggie DL, Jones C. Fluorescent imaging of the biliary tract during laparoscopic cholecystectomy. Ann Surg Innov Res. 2014;8:5.
Sakaguchi T, Suzuki A, Unno N, et al. Bile leak test by indocyanine green fluorescence images after hepatectomy. Am J Surg. 2010;200:19–23.
Ishizawa T, Tamura S, Masuda K, et al. Intraoperative fluorescent cholangiography using indocyanine green: a biliary road map for safe surgery. J Am Coll Surg. 2009;208:1–4.
Conflict of Interest
The authors declare that they have no competing interests. This study was funded by an educational grant from Karl Storz Endoscopy, Tuttlingen, Germany.
Compliance with Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study. Regarding informed consent being obtained from all individual participants for whom identifying information is included in this article, this does not apply.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dip, F., Nguyen, D., Montorfano, L. et al. Accuracy of Near Infrared-Guided Surgery in Morbidly Obese Subjects Undergoing Laparoscopic Cholecystectomy. OBES SURG 26, 525–530 (2016). https://doi.org/10.1007/s11695-015-1781-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-015-1781-9