
Abstract
Background
The goal of this study was to document the relationship between BMI and the components of bariatric surgical operating room (OR) time.
Methods
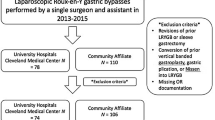
The Stanford Translational Research Integrated Database Environment identified all patients who underwent laparoscopic Roux-en-Y gastric bypass procedures at Stanford University Medical Center between May 2008 and November 2013. The 434 patients were divided into 3 groups: group 1 (n = 213) BMI ≥35 to <45 kg/m2, group 2 (n = 188) BMI ≥45.0 to <60 kg/m2, and group 3 (n = 33) BMI ≥60 kg/m2. The primary variable measured was total operating room time, defined as beginning when the patient entered the OR until the moment the patient physically left the OR. Secondary variables were anesthetic induction time, nursing preparation time, operation time, time for emergence from anesthesia, and total length of hospital stay.
Results
Increasing BMI was associated with increased total OR time (group 1 = 202 min, group 2 = 215 min, group 3 = 235 min), mainly due to longer operation time (group 1 = 147 min, group 2 = 154 min, group 3 = 163 min). Anesthetic induction (group 1 = 17 min, group 2 = 18 min, group 3 = 23 min) and emergence times (group 1 = 12 min, group 2 = 12 min, group 3 = 22 min) were also significantly longer in the largest patients.
Conclusions
Operating room schedules and plans for resource utilization should recognize that the same bariatric procedure will require more time for patients with BMI >60 kg/m2 than for smaller bariatric patients.






Similar content being viewed by others
References
Wang JL, Gadinsky NE, Yeager AM, et al. The increased utilization of operating room time in patients with increased BMI during primary total hip arthroplasty. J Arthroplasty. 2013;28(4):680–3. doi:10.1016/j.arth.2012.06.037.
Kadry B, Press CD, Alosh H, et al. Obesity increases operating room times in patients undergoing primary hip arthroplasty: a retrospective cohort analysis. Peer J. 2014;2:e530. doi:10.7717/peerj.530. eCollection 2014.
Lowe HJ, Ferris TA, Hernandez PM, et al. STRIDE—an integrated standards-based translational research informatics platform. AMIA Annu Symp Proc. 2009;2009:391–5.
Gupta PK, Franck C, Miller WJ, et al. Development and validation of a bariatric surgery risk calculator using prospective, multicenter NSQIP dataset. J Am Coll Surg. 2011;212(3):301–9. doi:10.1016/j.jamcollsurg.2010.11.003. Epub 2011 Jan 17.
Hlavac M. stargazer: LaTeX/HTML code and ASCII text for well-formatted regression and summary statistics tables. R package version 5.1. 2014. http://CRAN.R-project.org/package=stargazer.
Gottesfeld H. Body and self-cathexis of super-obese patients. J Psychosom Res. 1962;6:177–83.
Mason EE, Doherty C, Maher JW, et al. Super obesity and gastric reduction procedures. Gastroenterol Clin N Am. 1987;16(3):495–502.
World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i-xii, 1–253.
Renquist K. Obesity classification. Obes Surg. 1998;8(4):480.
NIH Consensus. Gastrointestinal surgery for severe obesity. National Institutes of Health Consensus Development Conference Draft Statement. Am J Clin Nutr. 1992 Feb;55(2 Suppl):615S-619S.
Sarr M, Felty C, Hilmer D, et al. Technical and practical considerations involved in operations on patients weighing more than 270 kg. Arch Surg. 1995;130(1):102–5.
Reames BN, Bacal D, Krell RW, et al. Influence of median surgeon operative duration on adverse outcomes in bariatric surgery. Surg Obes Relat Dis. 2014. doi:10.1016/j.soard.2014.03.018.
Stephens DJ, Saunders JK, Belsley S, et al. Short-term outcomes for super-super obese (BMI ≥ 60 kg/m2) patients undergoing weight loss surgery at a high-volume bariatric surgery center: laparoscopic adjustable gastric banding, laparoscopic gastric bypass, and open tubular gastric bypass. Surg Obes Relat Dis. 2008;4(3):408–15. doi:10.1016/j.soard.2007.10.013.
Hawn MT, Bian J, Leeth RR, et al. Impact of obesity on resource utilization for general surgery procedures. Ann Surg. 2005;241(5):821–6. discussion 826–8.
Farkas DT, Moradi D, Moaddel D, et al. The impact of body mass index on outcomes after laparoscopic cholecystectomy. Surg Endosc. 2012;26:964–9.
Gupta PK, Miller WJ, Sainath J, et al. Determinants of resource utilization and outcomes in laparoscopic Roux-en Y gastric bypass: a multicenter analysis of 14,251 patients. Surg Endosc. 2011;25(8):2613–25. doi:10.1007/s00464-011-1612-6.
Leykin Y, Pellis T, Del Mestro E, et al. Anesthetic management of morbidly obese and super-morbidly obese patients undergoing bariatric operations: hospital course and outcomes. Obes Surg. 2006;16:1563–9.
Brodsky JB, Lemmens HJM. Invited commentary: is the super-obese patient different? Obes Surg. 2006;16(12):1563–9.
Macario A. What does one minute of operating room time cost? J Clin Anesth. 2010;22(4):233–6. doi:10.1016/j.jclinane.2010.02.003.
Silber JH, Rosenbaum PR, Kelz RR, et al. Medical and financial risks associated with surgery in the elderly obese. Ann Surg. 2012;256(1):79–86. doi:10.1097/ SLA. 0b013e31825375ef.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
For this kind of retrospective study, the Stanford University School of Medicine IRB does not require informed consent. There was no patient identifying information in this manuscript.
Human and Animal Rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
Joseph A. Sanford is a Fellow of the Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University Medical Center, and holds a MD degree.
Bassam Kadry is a Professor at the Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University Medical Center, and holds a MD degree.
Jay B. Brodsky is a Professor at the Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University Medical Center, and holds a MD degree.
Alex Macario is a Professor at the Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University Medical Center, and holds a MD and MBA degree.
Rights and permissions
About this article

Cite this article
Sanford, J.A., Kadry, B., Brodsky, J.B. et al. Bariatric Surgery Operating Room Time—Size Matters. OBES SURG 25, 1078–1085 (2015). https://doi.org/10.1007/s11695-015-1651-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-015-1651-5