
Abstract
Background
Bariatric weight loss essentially is expressed with reference to the baseline weight, for example, as relative percentages or as absolute body mass index (BMI) points lost from baseline. A different definition of baseline weight would therefore affect all weight loss results. We try to determine which value to prefer for baseline weight in weight loss surgery: the accidental weight at time of operation or the patient-specific steady weight, reflecting a steady personal craving for calories that is independent of the operation.
Methods
Nadir percentage alterable weight loss (%AWL) outcome of all primary gastric bypass patients in our hospital with a 2-year follow-up is compared twice with nadir %AWL outcome of all revision gastric banding-to-bypass patients: relative to their BMI before their banding and before their banding-to-bypass (Mann-Whitney; p < 0.05).
Results
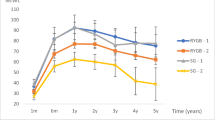
Out of 713 gastric bypass patients with a 2-year follow-up, 82 had revision banding-to-bypass. Total mean baseline BMI is 44.1 kg/m2; nadir BMI is 29.2 kg/m2. Difference in mean nadir weight loss between primary (49.4 %AWL) and revision patients is not significant if compared to baseline BMI before gastric banding (47.4 %AWL) but significant if compared to baseline BMI before revision banding-to-bypass (37.7 %AWL).
Conclusions
Revision gastric bypass with removal of gastric banding does not affect the “new” weight after the gastric banding but the “old” weight before the banding. Gastric bypass effectiveness was not added to the gastric banding effectiveness; it replaced it. Therefore, the patient-specific steady weight should be preferred for baseline BMI, reflecting an underlying personal craving for calories that remains constant over time and independent of a bariatric procedure. Baseline BMI can be standardized by using the measured weight at first visit before the primary bariatric procedure, also in revision cases.


Similar content being viewed by others


References
Benoit SC, Hunter TD, Francis DM, et al. Use of bariatric outcomes longitudinal database (BOLD) to study variability in patient success after bariatric surgery. Obes Surg. 2014;24(6):936–43.
Courcoulas AP, Christian NJ, Belle SH, et al. Weight change and health outcomes at 3 years after bariatric surgery among individuals with severe obesity. JAMA. 2013;310(22):2416–25.
Sjöström L, Peltonen M, Jacobson P, et al. Bariatric surgery and long-term cardiovascular events. JAMA. 2012;307(1):56–65.
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122(3):248–56.
Livhits M, Mercado C, Yermilov I, et al. Preoperative predictors of weight loss following bariatric surgery: systematic review. Obes Surg. 2012;22(1):70–89.
van de Laar AW. Algorithm for weight-loss after gastric-bypass surgery considering body mass index, gender, and age from the Bariatric Outcome Longitudinal Database (BOLD). Surg Obes Relat Dis. 2014;10(1):55–61.
Tabone LE. Comment on: algorithm for weight-loss after gastric-bypass surgery considering body mass index, gender, and age from the bariatric outcome longitudinal database. Surg Obes Relat Dis. 2014;10(1):61–3.
van de Laar AW, Dollé MH, de Brauw LM, et al. Validating the alterable weight-loss (AWL) metric with two year weight-loss outcome of 500 patients after gastric-bypass. Obes Surg. 2014. doi:10.1007/s11695-014-1203-4.
van de Laar AW, Acherman YI. Weight-loss percentile charts of large representative series: a benchmark defining sufficient weight-loss challenging current criteria for success of bariatric surgery. Obes Surg. 2013. doi:10.1007/s11695-013-1130-9.
The committee on standards for reporting results, Mason EE, Amaral J, et al. Standards for reporting results. Obes Surg. 1994;4(1):56–65.
Sjöström L, Narbro K, Sjöström C, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357(8):741–52.
Christou N, Efthimiou E. Five-year outcomes of laparoscopic adjustable gastric-banding and laparoscopic Roux-en-Y gastric-bypass in a comprehensive bariatric surgery program in Canada. Can J Surg. 2009;52:249–58.
Deitel M, Gawdat K, Melissas J. Reporting weight-loss 2007. Obes Surg. 2007;14:565–8.
Faria G, Preto J, Almeida AB, et al. Fasting glycemia: a good predictor of weight-loss after RYGB. Surg Obes Relat Dis. 2013. doi:10.1016/j.soard.2013.11.005.
Adams ST, Salhab M, Hussain ZI, et al. Roux-en-Y gastric-bypass for morbid obesity: what are the preoperative predictors of weight-loss? Postgrad Med J. 2013;89(1053):411–6.
Ortega E, Morínigo R, Flores L, et al. Predictive factors of excess body weight-loss 1 year after laparoscopic bariatric surgery. Surg Endosc. 2012;26(6):1744–50.
Perugini RA, Mason R, Czerniach DR, et al. Predictors of complication and suboptimal weight-loss after laparoscopic Roux-en-Y gastric-bypass: a series of 188 patients. Arch Surg. 2003;138(5):541–5.
van de Laar A. Bariatric Outcomes Longitudinal Database (BOLD) suggests excess weight loss and excess BMI loss to be inappropriate outcome measures, demonstrating better alternatives. Obes Surg. 2012;22(12):1843–7.
Conflict of Interest
The authors Arnold van de Laar, Marije Dollé, Maurits de Brauw, Sjoerd Bruin, and Yair Acherman declare that they have no conflict of interest.
Informed consent was obtained from all individual participants included in the study.
For this type of study (retrospective studies), formal consent is not required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
van de Laar, A.W., Dollé, M.H., de Brauw, L.M. et al. Which Baseline Weight Should Be Preferred as Reference for Weight Loss Results? Insights in Bariatric Weight Loss Mechanisms by Comparing Primary and Revision Gastric Bypass Patients. OBES SURG 25, 687–693 (2015). https://doi.org/10.1007/s11695-014-1438-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1438-0