
ABSTRACT
BACKGROUND
Patient hand-offs at physician shift changes have limited ability to convey the primary team’s longitudinal insight. The Patient Acuity Rating (PAR) is a previously validated, 7-point scale that quantifies physician judgment of patient stability, where a higher score indicates a greater risk of clinical deterioration. Its impact on cross-covering physician understanding of patients is not known.
OBJECTIVE
To determine PAR contribution to sign-outs.
DESIGN
Cross-sectional survey.
SUBJECTS
Intern physicians at a university teaching hospital.
INTERVENTIONS
Subjects were surveyed using randomly chosen, de-identified patient sign-outs, previously assigned PAR scores by their primary teams. For each sign-out, subjects assigned a PAR score, then responded to hypothetical cross-cover scenarios before and after being informed of the primary team’s PAR.
MAIN MEASURE
Changes in intern assessment of the scenario before and after being informed of the primary team’s PAR were measured. In addition, responses between novice and experienced interns were compared.
KEY RESULTS
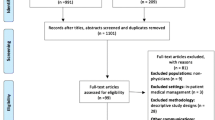
Between May and July 2008, 23 of 39 (59 %) experienced interns and 25 of 42 (60 %) novice interns responded to 480 patient scenarios from ten distinct sign-outs. The mean PAR score assigned by subjects was 4.2 ± 1.6 vs. 3.8 ± 1.8 by the primary teams (p < 0.001). After viewing the primary team’s PAR score, interns changed their level of concern in 47.9 % of cases, their assessment of the importance of immediate bedside evaluation in 48.7 % of cases, and confidence in their assessment in 43.2 % of cases. For all three assessments, novice interns changed their responses more frequently than experienced interns (p = 0.03, 0.009, and <0.001, respectively). Overall interns reported the PAR score to be theoretically helpful in 70.8 % of the cases, but this was more pronounced in novice interns (81.2 % vs 59.6 %, p < 0.001).
CONCLUSIONS
The PAR adds valuable information to sign-outs that could impact cross-cover decision-making and potentially benefit patients. However, correct training in its use may be required to avoid unintended consequences.



Similar content being viewed by others


REFERENCES
Petersen LA, Brennan TA, O’Neil AC, Cook EF, Lee TH. Does housestaff discontinuity of care increase the risk for preventable adverse events? Ann Intern Med. 1994;121(11):866–72.
Vidyarthi AR. Fumbled handoff. AHRQ Web M & M. March 2004. Available at: http://webmm.ahrq.gov/case.aspx?caseID=55. Accessed: October 4, 2012.
Singh H, Thomas EJ, Petersen LA, Studdert DM. Medical errors involving trainees: a study of closed malpractice claims from 5 insurers. Arch Intern Med. 2007;167(19):2030–6.
Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004;79(2):186–94.
Arora V, Johnson J, Lovinger D, Humphrey HJ, Meltzer DO. Communication failures in patient sign-out and suggestions for improvement: a critical incident analysis. Qual Saf Health Care. 2005;14(6):401–7.
Borowitz SM, Waggoner-Fountain LA, Bass EJ, Sledd RM. Adequacy of information transferred at resident sign-out (in-hospital handover of care): a prospective survey. Qual Saf Health Care. 2008;17(1):6–10.
Horwitz LI, Krumholz HM, Green ML, Huot SJ. Transfers of patient care between house staff on internal medicine wards: a national survey. Arch Intern Med. 2006;166(11):1173–7.
Solet DJ, Norvell JM, Rutan GH, Frankel RM. Lost in translation: challenges and opportunities in physician-to-physician communication during patient handoffs. Acad Med. 2005;80(12):1094–9.
Vidyarthi AR, Arora V, Schnipper JL, Wall SD, Wachter RM. Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign-out. J Hosp Med. 2006;1(4):257–66.
Horwitz LI, Moin T, Krumholz HM, Wang L, Bradley EH. Consequences of inadequate sign-out for patient care. Arch Intern Med. 2008;168(16):1755–60.
Chang VY, Arora VM, Lev-Ari S, D’Arcy M, Keysar B. Interns overestimate the effectiveness of their hand-off communication. Pediatrics. 2010;125(3):491–6.
Horwitz LI, Moin T, Green ML. Development and implementation of an oral sign-out skills curriculum. J Gen Intern Med. 2007;22(10):1470–4.
Accreditation Council for Graduate Medical Education (ACGME). Task Force on Quality Care and Professionalism. Proposed Standards: Common Program Requirements. 2010. Available at: http://www.acgme-2010standards.org/pdf/Common_Program_Requirements_07012011.pdf. Accessed: October 4, 2012.
Byrne A. Mental workload as a key factor in clinical decision making. Adv Health Sci Educ Theory Pract. 2012. doi:10.1007/s10459-012-9360-5.
Hodgetts TJ, Kenward G, Vlachonikolis IG, Payne S, Castle N. The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team. Resuscitation. 2012;54(2):125–31.
Edelson DP, Retzer E, Weidman EK, Woodruff J, Davis AM, Minsky BD, et al. Patient acuity rating: quantifying clinical judgment regarding inpatient stability. J Hosp Med. 2011;6(8):475–9.
Hirschtick RE. A piece of my mind. Copy-and-paste. JAMA. 2006;295(20):2335–6.
Wohlauer MV, Arora VM, Horwitz LI, Bass EJ, Mahar SE, Philibert I. The patient handoff: a comprehensive curricular blueprint for resident education to improve continuity of care. Acad Med. 2012;87(4):411–8.
Norman G, Young M, Brooks L. Non-analytical models of clinical reasoning: the role of experience. Med Educ. 2007;41(12):1140–5.
Bachmann LM, Muhleisen A, Bock A, ter Riet G, Held U, Kessels AG. Vignette studies of medical choice and judgment to study caregivers’ medical decision behaviour: systematic review. BMC Med Res Methodol. 2008;8:50.
Cooksey RW. Judgment Analysis: theory, Methods, and Applications. San Diego: Academic; 1996.
Acknowledgments
Contributors
We would like to thank Elizabeth Weidman and Jefferson Cua for their help in data collection and entry, Seo Young Park, PhD for statistical support, and Cara V. Phillips for graphics support.
Funders
This study was supported by the National Heart, Lung, and Blood Institute (K23 HL097157-01; PI: Edelson) and by a National Institute of Aging (5 T35 AG029795-02) grant for the Pritzker Summer Research Program.
Registry Number
clinicaltrials.gov NCT01082991
Prior Presentations
Prior poster presentation at the 2009 Society of Hospital Medicine Annual Meeting in Chicago, IL.
Conflict of Interest
Dr. Arora has received research support from Picker Institute (Grant #86) and National Institute of Aging (K23 AG033763), and is the on editorial board of Agency for Healthcare Research and Quality Web M&M. Dr. Edelson has received research support from the National Heart, Lung, and Blood Institute (K23 HL097157-01; PI: Edelson). Dr. Philips, Mr. Yuen, Dr. Retzer, and Dr. Woodruff declare they have no conflict of interests
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 68 kb)
Rights and permissions
About this article
Cite this article
Phillips, A.W., Yuen, T.C., Retzer, E. et al. Supplementing Cross-Cover Communication with the Patient Acuity Rating. J GEN INTERN MED 28, 406–411 (2013). https://doi.org/10.1007/s11606-012-2257-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-012-2257-4