
Abstract
Introduction
Esophagocoloplasty represents a useful technique to restore the intestinal continuity after esophagogastrectomy. This technique has been used mainly after esophagogastric caustic injuries. The aim of this review is to assess the role of esophagogastrectomy with esophagocoloplasty for esophageal or gastric neoplasms.
Methods
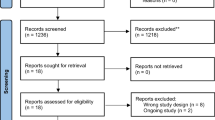
A systematic literature search was performed using Embase, Medline, Cochrane, and PubMed databases to identify all studies published in the previous 25 years (1991–2016) reporting cases of esophagocoloplasty after esophagogastrectomy for malignancies. The systematic review was conducted according to the PRISMA guidelines.
Results
The systematic review of the literature shows a morbidity rate of 57% and a mortality rate of 15% in the 93 reported cases of esophagocoloplasty performed for malignant diseases. However, R0 rate ranged from 76.1 to 85%, and 5-year survival was obtained in 11.9–32.8% of patients in the different series.
Conclusions
In highly selected cases of primary or relapsing gastric or esophageal neoplasms, esophagogastrectomy with esophagocoloplasty is a viable and useful option, which may guarantee complete tumor resection and long-term survival.


Similar content being viewed by others


References
Chirica M, Brette MD, Faron M, Munoz Bongrand N, Halimi B, Laborde C, Sarfati E, Cattan P. Upper digestive tract reconstruction for caustic injuries. Ann Surg 2015;261:894–901.
Chirica M, Vuarnesson H, Zohar S, Faron M, Halimi B, Munoz Bongrand N, Cattan P, Sarfati E. Similar outcomes after primary and secondary esophagocoloplasty for caustic injuries. Ann Thorac Surg. 2012;93(3):905–12. doi: 10.1016/j.athoracsur.2011.12.054
Pompeo E, Nofroni I, Van Raemdonck D, Coosemans W, Van Cleynenbreughel B, Lerut T. Esophagocoloplasty for congenital, benign and malignant diseases. Surgical and long-term functional results. Eur J Cardiothorac Surg 1996;10:561–7.
Boukerrouche A. Left colonic graft in esophageal reconstruction for caustic stricture: mortality and morbidity. Dis Esophagus 2013;26:788–93.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009, 151:264–9.
The Cochrane Collaboration’s tool for assessing risk of bias. http://ohg.cochrane.org/sites/ohg.cochrane.org/files/uploads/Risk%20of%20bias%20assessment%20tool.pdf. Accessed March 7, 2016.
Butte JM, Waugh E, Parada H, De La Fuente H. Combined total gastrectomy, total esophagectomy, and D2 lymph node dissection with transverse colonic interposition for adenocarcinoma of the gastroesophageal junction. Surg Today 2011;41:1319–23.
Ceroni M, Norero E, Henríquez JP, Viñuela E, Briceño E, Martínez C, Aguayo G, Araos F, González P, Díaz A, Caracci M. Total esophagogastrectomy plus extended lymphadenectomy with transverse colon interposition: a treatment for extensive esophagogastric junction cancer. World J Hepatol 2015;7:2411–7.
Andreollo NA, Coelho Neto Jde S, Calomeni GD, Lopes LR, Tercioti Junior V. Total esophagogastrectomy in the neoplasms of the esophagus and esofagogastric junction: when must be indicated? Rev Col Bras Cir 2015;42:360–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
ESM 1
(M4 V 79426 kb)
Rights and permissions
About this article

Cite this article
Aurello, P., Petrucciani, N., Sirimarco, D. et al. Esophagectomy with Esophagocoloplasty for Malignancies: Indications, Technique (with Video), and Results. Systematic Review of the Literature. J Gastrointest Surg 21, 1557–1561 (2017). https://doi.org/10.1007/s11605-017-3449-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-017-3449-3