
Abstract
This review aims to identify the optimal exercise intervention characteristics for falls prevention among community-dwelling adults aged 60 years and over. Articles for inclusion were sourced by searching the Academic Search Premier, AMED, Biomedical Reference Collection: Expanded, CINAHL Plus, MEDLINE and SPORTDiscus databases with the key words ‘falls’, ‘prevention’, ‘exercise’ and ‘community’ and via reference lists of relevant articles. Only articles of level 1 or level 2 evidence (Howick et al. 2011) were included. Other inclusion criteria included recording falls incidence as an outcome measure, examining a community-dwelling population aged 60 years or over and implementing exercise as a single intervention in at least one group. Exercise programme characteristics from 31 articles were examined according to their frequency, intensity, time and type and their effects on falls incidence were reviewed. Exercising for a minimum of 1 h/week for at least 40 h over the course of an intervention is required to successfully reduce falls incidence. The optimal exercise frequency is three times per week, but the optimal duration per bout remains unclear. Specific balance training of sufficiently challenging intensity is a vital programme component, and strength training is most effective when combined with balance training. Flexibility and endurance training may also be included as part of a comprehensive programme. A combination of group and individual home exercise may be most effective for preventing falls and promoting exercise adherence.
Similar content being viewed by others

Introduction
Falls are prevalent among community-dwelling older adults. Approximately one in four people aged 65 years and over fall annually, with this proportion increasing to almost one in two among those aged 85 years and over [36]. Approximately 5 % of falls result in fractures or hospitalisation [46], and the long-term consequences of falling can be severe: a single fall can increase an older person’s risk of admission to a nursing home within 12 months by four to five times, while multiple falls can more than double the risk of death within 12 months [18, 59].
Falls are a global concern. In the USA, falls are the leading cause of fatal and non-fatal injuries to those aged over 65 years [11]. European data indicate that the economic burden owing to falls is substantial. In the UK, the annual cost of falls among those aged 60 and over was estimated at £981 million in 1999 [49]. In Ireland, the cost of falls to the Health Service Executive was estimated to be €400 million in 2006 and is projected to increase to €1 billion by 2020 [24]. As such, it is clear that effective, low-cost interventions to prevent falls must be implemented.
A range of single interventions, including exercise [9], environmental modification [15] and psychotropic medication withdrawal [7], as well as multifactorial interventions [12, 16], has been found to prevent falls. Exercise is the most widely investigated and effective single intervention for reducing both the rate and risk of falls [6, 14, 21]. Exercise alone is as effective as multifactorial intervention in reducing falls incidence and is frequently included as a component in effective multifactorial programmes [16, 34, 58].
However, exercise programme characteristics vary between studies and are often not clearly described in studies of multifactorial interventions. Recent guidelines from the American and British Geriatrics Societies [54] state that exercise is an essential intervention for preventing falls in community-dwelling older adults, but do not recommend precise exercise characteristics for this purpose. This presents a challenge to clinicians wishing to design and implement an effective evidence-based exercise programme for an individual that is at risk of falling. As identified by Arnold et al. [1], there is a need to clarify the optimum frequency, intensity, type and duration of exercise for falls prevention.
Sherrington et al. [50, 51] have conducted systematic reviews and meta-analyses to determine the effects of exercise on falls and to identify determinants of these effects. Their findings produced valuable recommendations concerning the type, dose and settings of exercise which are associated with greater effectiveness, but these recommendations are based on evidence from older adults both in the community and in residential care. Since older adults’ fall risk profiles and levels of physical function vary according to residential status [48], this review aims to examine the literature pertaining to community-dwelling older adults only in order to identify the optimum features of an exercise intervention to target that group’s specific risk factors [54]. These features will be described in terms of the FITT principle, i.e. the frequency of exercise, the target intensity, the time spent exercising and the type(s) of exercise undertaken [25]. Exercise adherence was also not addressed in previous reviews. Since poor uptake and adherence will render an intervention ineffective regardless of the programme design and content [40], factors relating to exercise programme adherence will be identified and discussed in this review also. By emphasising practical factors relating to exercise programme content, delivery and adherence, the overriding goal of this review is to facilitate clinicians who wish to design and implement an effective, evidence-based, targeted intervention for clients in this population.
Method
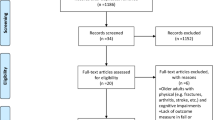
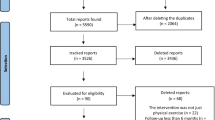
The literature search was conducted in June 2011. The databases searched for articles for inclusion were Academic Search Premier, AMED, Biomedical Reference Collection: Expanded, CINAHL Plus, MEDLINE and SPORTDiscus with the key words ‘falls’, ‘prevention’, ‘exercise’ and ‘community’. Reference lists of relevant articles were also searched. The initial search yielded 518 articles. A seven-step screening process was used to determine the eligibility of articles for review (Fig. 1). The seven exclusion criteria were as follows:
-
1.
Duplicate articles
-
2.
Articles of lower than level 1 or level 2 evidence, as determined by the Oxford Centre for Evidence-Based Medicine [26]
-
3.
Articles that were not full-text peer-reviewed publications
-
4.
Articles not available in English
-
5.
Studies that did not include falls as an outcome measure
-
6.
Studies of populations with specific medical conditions only or populations other than community-dwelling older adults
-
7.
Studies that did not employ exercise as a single intervention in at least one group

Flow chart illustrating the literature search and screening process
Although the purpose of this review was to examine the evidence relating to exercise interventions only, studies in which falls prevention education was provided in the manner of a population-based health promotion intervention, i.e. posters, pamphlets, etc., were also included, as it is not possible to categorically state that any group would not be exposed to such information.
Results
Table 1 lists the 31 studies reviewed and provides detail on study design and aspects of methodological quality. Two papers [17, 19] have been summarised as one throughout this review, as they describe the same trial, but reported using differing statistical methods. Table 2 summarises the characteristics of the exercise programmes studied and their influences on falls. Table 3 provides details of the types of exercise included in each programme according to the ProFaNE taxonomy [31].
Discussion
Frequency
Exercise frequency in the studies reviewed predominantly ranged from once per week to daily exercise. Exercising once per week appears to be inadequate for falls prevention, with only one pilot study reporting a short-term reduction in falls incidence at that frequency [65], although it may be sufficient to produce some balance and functional improvements [39]. The minimum effective frequency reported was twice per week [61], although this effect was noted in the short term only and was not supported by studies of longer duration [10, 22, 35]. Exercising three times per week was the most commonly adopted and most consistently effective approach across the studies reviewed [4, 8, 9, 27, 33, 37, 43, 44, 47, 53, 56, 64]. Where effects were non-significant, some instances of trends towards reductions in falls rates were observed [52, 63]. In other cases, additional factors such as exercise type and intensity may have been influential [29, 32, 42].
Mixed evidence was observed for programmes involving more frequent exercise. Studies aiming for daily exercise reduced falls rates by approximately 21–47 % [2, 17, 28, 30, 62], although adherence to the desired frequency was poor. After 1 year, Barnett et al. [2] found that only 13 % of participants were exercising daily at home, with the vast majority (91 %) exercising just once per week outside of group exercise classes. Similarly, the participants of Day et al. [17] reported exercising approximately twice per week outside of group sessions. This suggests that very high exercise frequencies may not be acceptable to older adults, but further supports the finding that exercising three times per week is effective. These findings confirm those of Costello and Edelstein [14] by indicating that the optimum frequency of exercise for falls prevention is three times per week, since it allows significant benefits to be attained while remaining acceptable to this population.
Intensity
Clear guidelines exist describing appropriate strength and endurance training intensities for older adults [38]. Many studies stated that their programmes met these guidelines in relation to one or both types of training [4, 30, 32, 35, 47], but most did not provide sufficient detail of exercise intensity. All studies in which guideline intensities were explicitly not met did not significantly reduce falls incidence [28, 29, 42, 55]. This highlights that strengthening and endurance exercise must be of an appropriate intensity to achieve training effects and the ensuing clinical benefits.
Defining an optimal intensity for balance training is problematic, since there is currently no standard measure by which to express the balance training intensity. Thus, its reporting in the studies reviewed was vague and inconsistent, with descriptions including ‘demanding’ [17], ‘challenging’ [53] and of ‘appropriate and increasing levels of difficulty’ [9] being used. Sherrington et al. [51] categorised balance training intensity according to the presence or absence of certain components: moving the body’s centre of mass, reducing the base of support and minimising upper limb support. Based on these criteria, the majority of reviewed studies which included balance training may be classified as ‘highly challenging’.
Progression of intensity is vital for continuing training gains to be obtained, but maintaining safety while providing adequate challenge is essential. Costello and Edelstein [14] proposed that balance training should therefore be conducted at the highest possible level of difficulty without falling or near-falling to ensure sufficient training intensity, and that each exercise should be mastered before progressing to ensure safety. Structured programmes such as the Otago Exercise Programme (OEP) [8, 9, 43, 44] provide a useful framework for clinicians to prescribe and progress balance training, although these principles have been adopted effectively in less rigidly structured programmes without adverse events [17, 19, 37, 61].
Time
Time spent exercising may be considered in numerous ways: the duration of each exercise bout, the duration of the intervention or the total exercise volume, i.e. the cumulative time spent exercising throughout an intervention. The duration of a single bout of exercise varied from approximately 15 to 120 min in the studies reviewed. No consistent relationship between bout duration and the effectiveness of an intervention was observed, although the majority of effective interventions included some bouts of at least 60 min or more. Bouts of longer durations, i.e. 90–120 min in length, were all conducted in group settings—including time for explanation, demonstration, etc.—rather than as single, continuous bouts of exercise.
The total duration of the exercise programmes varied greatly. Effective interventions lasted from 5 weeks [61] to 2 years [8]. The most commonly observed programme durations were from 15 weeks to 12 months. Most interventions of approximately 4 months duration were reported to reduce falls [17, 19, 28, 62], while 12-month interventions reduced—or showed trends towards reducing—falls incidence [2, 9, 33, 43, 44, 52, 64, 65], with some exceptions [35, 42, 63]. The length of follow-up must be considered as a potential source of bias in short-term studies. Reporting the immediate effects of short-term interventions may show reductions in falls incidence, but falls may occur infrequently, thus participants must be observed over an extended time period to detect true changes. Some evidence suggests that the effects of shorter interventions may be carried over to long-term follow-up [56, 61], while the results of Yamada et al. negate this [65]. Further research investigating participants’ continuing exercise behaviours upon completion of short-term interventions is required.
Total exercise volume also varied; even among interventions of equal duration, e.g. tai chi group of Wolf et al. [62] spent 64 h exercising compared to approximately 11 h for the balance training group, despite both interventions lasting 15 weeks. To overcome the challenge this presents in comparing interventions, it may be helpful to consider the exercise volume per week for each intervention (Table 2). When considered in this manner, all effective interventions were found to involve at least 1 h of exercise per week. Ineffective interventions that exceeded this volume were noted to have insufficient exercise frequency [10, 22, 35], questionable exercise intensity [20, 42, 55, 63] or involve exercise of an inappropriate type [29, 32], with the exception of the intervention of Shumway-Cook et al. [52] which displayed a trend towards significant falls reduction. Overall, effective interventions comprised of at least 40 h of exercise over the course of the intervention, slightly less than the cutoff of 50 h suggested previously [50, 51]. Interventions with high exercise volumes [33, 52] were reasonably successful, but cited poor adherence as a barrier to further success. The OEP involves approximately half the volume of exercise of that prescribed by Shumway-Cook et al. [52] and is successful in both preventing falls and gaining adherence [57]. Thus, while no definitive total exercise volume can be recommended, it is apparent that exercise programmes must meet certain minimum requirements while remaining acceptable to participants to be effective.
Type
Guidelines recommend a comprehensive programme of balance, strength, endurance and flexibility training for all adults aged 65 and over [38]. A number of the studies reviewed implemented such a programme with the effect of reducing falls incidence [2, 20, 30, 65], including the OEP which reduced fall rates and fall-related injuries by approximately 32 % [57]. Similarly, the 36-week FaME programme [53] delivered a home programme based on the OEP combined with a supervised exercise class which included more challenging balance exercises. This intervention produced a similar immediate reduction in falls rates, increasing to 54 % after 1 year, suggesting additional benefits from group classes and more challenging balance training.
Freiberger et al. [20] investigated the optimum amount of emphasis to place on each component of a comprehensive programme. Although it did not reach significance, their fitness group—in which strength/flexibility, balance and endurance training each comprised 33 % of the programme—experienced a trend towards a reduction in falls incidence, while the psychomotor group—in which strength and balance combined comprised just 40 % of the programme—did not. Similarly, Day et al. [17] observed a reduction in falls incidence and improvements in balance with a comprehensive programme which is comprised of 30–35 % balance training. These results suggest that balance training should constitute at least one third of the total programme content and be given at least equal emphasis compared to other components for optimum fall prevention.
The nature of balance training undertaken varied between studies, although training principles remained similar. Exercises which encouraged reducing or leaning beyond the base of support, shifting the body’s centre of mass, minimising upper limb support, coordinating single or dual-task movements, altering sensory feedback and functional activities were commonly used in balance training. Some effective novel approaches included computerised balance training [62], group games [39, 47] and obstacle courses [47, 61]. Tai chi was also consistently successful in preventing falls and appears to be an effective method of integrating many principles of balance training into one accessible programme [27, 33, 56, 62–64].
Certain characteristics were common to ineffective programmes: firstly, the lack of a balance training component [32, 63]. Secondly, programmes which lacked functional relevance were ineffective [29, 32]. Finally, programmes which lacked exercise progression were also ineffective in preventing falls [42].
The inclusion of walking in falls prevention exercise programmes has been identified as a contentious issue, with suggestions that walking may increase fall-risk exposure and reduce the emphasis on vital balance training [51]. In the studies reviewed which included a walking component [2, 8, 9, 20, 30, 43, 44, 47, 65], walking was not consistently associated with the effectiveness of the intervention. However, Rubenstein et al. [47] showed some association between exercise—which included walking—and increased falls risk. Clinicians may identify individuals who are at high risk of falling and would be unsafe undertaking a walking programme independently and chose not to recommend walking in such cases, an approach adopted in the OEP and supported by Sherrington et al. [50]. Other lower risk forms of endurance training, e.g. stationary cycling, swimming, etc., may be substituted if desired.
Delivery and adherence
Shumway-Cook et al. [52] demonstrated the importance of adherence to the success of a falls prevention programme, with those who attended more than 75 % of exercise classes having 41 % fewer falls than those who attended less than 33 % of classes. How best to ensure adherence remains unclear, although methods of exercise programme delivery may be influential.
Although a uniform population was targeted, various settings were observed for the exercise interventions reviewed, most commonly community centres and participants’ homes. Exercise in either location was effective, as were combined centre- and home-based programmes. A convenient location and accessibility via transport links are vital, as these were cited by participants as major contributing factors to dropping out of a programme [39]. However, Day et al. [17] provided transport for their participants to attend exercise classes, yet 26 % of participants never attended a class, and only 61 % attended more than half of their sessions. In addition, participants’ adherence to the recommended daily home exercise programme was poor despite being able to complete this in their own homes. It is clear, therefore, that although location is undoubtedly influential, other factors strongly influence exercise uptake and adherence.
Supervision and format (i.e. individual/group sessions) may be two such factors. Supervised group exercise is thought to facilitate uptake and adherence due to the leadership, social support and social outlet provided [5]. However, empowering individuals and encouraging self-regulated behaviour change are recommended to gain long-term motivation and exercise participation [3, 45]. In the studies reviewed, a combined approach with supervised group exercise supplemented by an individual home exercise programme appeared to be a common and effective choice of intervention, potentially providing a beneficial mix of both approaches. Providing individualised home exercise programmes with limited one-on-one supervision, as in the OEP, may also allow similar benefits to be attained, but the cost-effectiveness of this approach does not compare well to group programmes [41]. A novel approach that aimed to achieve adherence and long-term behaviour change by embedding training activities into everyday tasks was also investigated in one pilot study with promising results [13]. Larger trials of this approach are required to determine its acceptability to older adults.
Programme characteristics can also influence adherence. A strong negative correlation between exercise bout duration and adherence has recently been demonstrated in older women [60] and must be considered when designing an exercise programme for older adults. Low exercise frequency and intensity have been cited as facilitators to programme participation [5], although—as discussed—minimum requirements must be attained for a programme to be effective. Interventions of 5–12 weeks duration achieved excellent uptake and adherence, while longer interventions were associated with poorer uptake and adherence. However, as already stated, no studies examined long-term exercise behaviours of older adults following completion of short-term falls prevention programmes; thus, it is not possible to ascertain whether shorter interventions can bring about long-term positive changes in exercise behaviour.
Limitations
Since this review focused on identifying optimum exercise programme characteristics, only studies which examined exercise as a single intervention were included. Thus, the effect of exercise as part of a multifactorial intervention has not been considered. However, a factorial study [17] demonstrated that exercise was effective singly and in combination with home hazard modification and vision correction. In fact, combining all three interventions was found to bring about the greatest reduction in falls rates. This indicates that—while effective alone—a comprehensive exercise programme is also a vital component of a successful multifactorial intervention.
In terms of outcome measurement, not all studies reviewed utilised prospective falls diaries or calendars to record falls incidence, despite this being the current gold standard in falls data collection [23]. This may lead to inaccuracy in reports of falls incidence rates where retrospective methods are used. It may also render comparison with studies using prospective methods invalid. Statistical methods used to report changes in falls incidence also varied, making direct comparison between studies challenging.
Conclusions
The findings of this review agree with current falls prevention guidelines which state that older adults at risk of falling should be offered an exercise programme incorporating balance, gait and strength training, with flexibility and endurance training as adjuncts [54]. Our findings agree with those of previous reviews [1, 14, 50, 51] on a number of aspects. Three times per week appears to be the optimal exercise frequency. Specific balance training at a sufficiently challenging intensity is vital for falls prevention. Strength training in combination with balance training is effective in preventing falls. Walking may expose older adults to greater fall-risk; thus, we recommend that clinicians consider other endurance training activities for individuals at high risk of falling. As in previous reviews, current evidence remains strongest for interventions involving on-going exercise for approximately 12 months.
However, a number of original findings and findings that differ from those of previous reviews were also identified. This review identified that balance training should constitute at least one third of the total programme content. The optimal duration of individual exercise bouts remains unclear, although some evidence to support the inclusion of bouts of approximately 60 min duration was noted. Longer bouts, e.g. 90–120 min, are most acceptable in group settings. Exercise volumes of at least 1 h per week, with a minimum of approximately 40 h of exercise accumulated over the course of an intervention, were found to significantly reduce falls incidence. We found mixed evidence as regards the effects of shorter interventions on long-term falls incidence; thus, further research into how such interventions affect long-term exercise behaviour and motivation is recommended. As noted in previous reviews, exercise can be effective when delivered in a variety of methods and settings. Our findings advocate that a combination of supervised group exercise in a convenient centre and individual home-based exercise is optimal for preventing falls while achieving psychosocial benefits which may support uptake and adherence. Adherence may be further supported by implementing programmes which incorporate the exercise characteristics discussed while minimising time demands for participants.
References
Arnold CM, Sran MM, Harrison EL (2008) Exercise for fall risk reduction in community-dwelling older adults: a systematic review. Physiother Can 60(4):358–372
Barnett A, Smith B, Lord S, Williams M, Baumand A (2003) Community-based group exercise improves balance and reduces falls in at-risk older people: a randomised controlled trial. Age Ageing 32(4):407–414
Brawley LR, Rejeski WJ, King AC (2003) Promoting physical activity for older adults: the challenges for changing behavior. Am J Prev Med 25 (3, Supplement 2):172–183
Buchner D, Cress M, de Lateur B, Esselman P, Margherita A, Price R, Wagner E (1997) The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J Gerontol 52A(4):M218–M224
Bunn F, Dickinson A, Barnett-Page E, McInnes E, Horton K (2008) A systematic review of older people’s perceptions of facilitators and barriers to participation in falls-prevention interventions. Ageing Soc. doi:10.1017/s0144686x07006861
Campbell AJ, Robertson MC (2007) Rethinking individual and community fall prevention strategies: a meta-regression comparing single and multifactorial interventions. Age Ageing 36(6):656–662
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Buchner DM (1999) Psychotropic medication withdrawal and a home-based exercise program to prevent falls: a randomized, controlled trial. J Am Geriatr Soc 47(7):850–853
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Buchner DM (1999) Falls prevention over 2 years: a randomized controlled trial in women 80 years and older. Age Ageing 28(6):513–518
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Tilyard MW, Buchner DM (1997) Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ 315(7115):1065–1069
Carter ND, Khan KM, McKay HA, Petit MA, Waterman C, Heinonen A, Janssen PA, Donaldson MG, Mallinson A, Riddell L, Kruse K, Prior JC, Flicker L (2002) Community-based exercise program reduces risk factors for falls in 65- to 75-year-old women with osteoporosis: randomized controlled trial. CMAJ 167(9):997–1004
Centers for Disease Control and Prevention (2011) Injury prevention & control: data & statistics (WISQARSTM). Available http://www.cdc.gov/injury/wisqars/index.html. Accessed 9 Mar 2011
Clemson L, Cumming RG, Kendig H, Swann M, Heard R, Taylor K (2004) The effectiveness of a community-based program for reducing the incidence of falls in the elderly: a randomized trial. J Am Geriatr Soc 52(9):1487–1494
Clemson L, Singh MF, Bundy A, Cumming RG, Weissel E, Munro J, Manollaras K, Black D (2010) LiFE pilot study: a randomised trial of balance and strength training embedded in daily life activity to reduce falls in older adults. Aust Occup Ther J 57(1):42–50
Costello E, Edelstein JE (2008) Update on falls prevention for community-dwelling older adults: review of single and multifactorial intervention programs. J Rehabil Res Dev 45(8):1135–1152
Cumming RG, Thomas M, Szonyi G, Salkeld G, O’Neill E, Westbury C, Frampton G (1999) Home visits by an occupational therapist for assessment and modification of environmental hazards: a randomized trial of falls prevention. J Am Geriatr Soc 47(12):1397–1402
Davison J, Bond J, Dawson P, Steen IN, Kenny RA (2005) Patients with recurrent falls attending accident & emergency benefit from multifactorial intervention: a randomised controlled trial. Age Ageing 34(2):162–168
Day L, Fildes B, Gordon I, Fitzharris M, Flamer H, Lord S (2002) Randomised factorial trial of falls prevention among older people living in their own homes. BMJ 325(7356):128
Donald IP, Bulpitt CJ (1999) The prognosis of falls in elderly people living at home. Age Ageing 28(2):121–125
Fitzharris MP, Day L, Lord SR, Gordon I, Fildes B (2010) The Whitehorse NoFalls trial: effects on fall rates and injurious fall rates. Age Ageing 39(6):728–733
Freiberger E, Menz HB, Abu-Omar K, Rutten A (2007) Preventing falls in physically active community-dwelling older people: a comparison of two intervention techniques. Gerontology 53(5):298–305
Gillespie LD, Robertson MC, Gillespie WJ, Lamb SE, Gates S, Cumming RG, Rowe BH (2009) Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. doi:10.1002/14651858.CD007146.pub2
Haines TP, Russell T, Brauer SG, Erwin S, Lane P, Urry S, Jasiewicz J, Condie P (2009) Effectiveness of a video-based exercise programme to reduce falls and improve health-related quality of life among older adults discharged from hospital: a pilot randomized controlled trial. Clin Rehabil 23(11):973–985
Hannan MT, Gagnon MM, Aneja J, Jones RN, Cupples LA, Lipsitz LA, Samelson EJ, Leveille SG, Kiel DP (2010) Optimizing the tracking of falls in studies of older participants: comparison of quarterly telephone recall with monthly falls calendars in the MOBILIZE Boston Study. Am J Epidemiol 171(9):1031–1036
Health Service Executive, National Council on Ageing and Older People, Department of Health and Children (2008) Strategy to prevent falls and fractures in Ireland’s ageing population. Dublin
Heyward VH (2010) Advanced fitness assessment and exercise prescription, 6th edn. Human Kinetics, Champaign
Howick J, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The Oxford 2011 levels of evidence. OCEBM Levels of Evidence Working Group. Oxford Centre for Evidence-Based Medicine, Oxford
Huang HC, Liu CY, Huang YT, Kernohan WG (2010) Community-based interventions to reduce falls among older adults in Taiwan: long time follow-up randomised controlled study. J Clin Nurs 19(7–8):959–968
Inokuchi S, Matsusaka N, Hayashi T, Shindo H (2007) Feasibility and effectiveness of a nurse-led community exercise programme for prevention of falls among frail elderly people: a multi-centre controlled trial. J Rehabil Med 39(6):479–485
Kamide N, Shiba Y, Shibata H (2009) Effects on balance, falls, and bone mineral density of a home-based exercise program without home visits in community-dwelling elderly women: a randomized controlled trial. J Physiol Anthropol 28(3):115–122
Kemmler W, von Stengel S, Engelke K, Haberle L, Kalender WA (2010) Exercise effects on bone mineral density, falls, coronary risk factors, and health care costs in older women: the randomized controlled senior fitness and prevention (SEFIP) study. Arch Intern Med 170(2):179–185
Lamb SE, Hauer K, Becker C (2007) Manual for the fall prevention classification system. Available http://www.profane.eu.org/documents/Falls_Taxonomy.pdf. Accessed 1 June 2011
Latham N, Anderson C, Bennett D, Stretton C (2003) Progressive resistance strength training for physical disability in older people. Cochrane Database Syst Rev (2):CD002759
Lin MR, Hwang HF, Wang YW, Chang SH, Wolf SL (2006) Community-based tai chi and its effect on injurious falls, balance, gait, and fear of falling in older people. Phys Ther 86(9):1189–1201
Logan PA, Coupland CA, Gladman JR, Sahota O, Stoner-Hobbs V, Robertson K, Tomlinson V, Ward M, Sach T, Avery AJ (2010) Community falls prevention for people who call an emergency ambulance after a fall: randomised controlled trial. BMJ 340:c2102
Lord SR, Tiedemann A, Chapman K, Munro B, Murray SM, Gerontology M, Ther GR, Sherrington C (2005) The effect of an individualized fall prevention program on fall risk and falls in older people: a randomized, controlled trial. J Am Geriatr Soc 53(8):1296–1304
Lord SR, Ward JA, Williams P, Anstey KJ (1993) An epidemiological study of falls in older community-dwelling women: the Randwick falls and fractures study. Aust J Public Health 17(3):240–245
Means KM, Rodell DE, O’Sullivan PS (2005) Balance, mobility, and falls among community-dwelling elderly persons: effects of a rehabilitation exercise program. Am J Phys Med Rehabil 84(4):238–250
Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, Macera CA, Castaneda-Sceppa C (2007) Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 116(9):1094–1105
Nitz JC, Choy NL (2004) The efficacy of a specific balance-strategy training programme for preventing falls among older people: a pilot randomised controlled trial. Age Ageing 33(1):52–58
Nyman SR, Victor CR (2011) Older people’s participation in and engagement with falls prevention interventions in community settings: an augment to the Cochrane systematic review. Age Ageing. doi:10.1093/ageing/afr103
Rankin J (2009) ACC pulls fall plan support. Manawatu Standard. Available at: http://www.stuff.co.nz/national/health/3000214/ACC-pulls-fall-plan-support Accessed 10 Oct 2011
Reinsch S, MacRae P, Lachenbruch PA, Tobis JS (1992) Attempts to prevent falls and injury: a prospective community study. Gerontologist 32(4):450–456
Robertson MC, Devlin N, Gardner MM, Campbell AJ (2001) Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 1: randomised controlled trial. BMJ 322(7288):697–701
Robertson MC, Gardner MM, Devlin N, McGee R, Campbell AJ (2001) Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 2: controlled trial in multiple centres. BMJ 322(7288):701–704
Robinson L, Dawson P, Newton J (2008) Promoting adherence with exercise-based falls prevention programmes. In: Vincent ML, Moreau TM (eds) Accidental falls: causes, prevention and intervention. Nova, New York, pp 283–298
Rubenstein LZ (2006) Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing 35(Suppl 2):ii37–ii41
Rubenstein LZ, Josephson KR, Trueblood PR, Loy S, Harker JO, Pietruszka FM, Robbins AS (2000) Effects of a group exercise program on strength, mobility, and falls among fall-prone elderly men. J Gerontol A Biol Sci Med Sci 55(6):M317–321
Scott V, Votova K, Scanlan A, Close J (2007) Multifactorial and functional mobility assessment tools for fall risk among older adults in community, home-support, long-term and acute care settings. Age Ageing 36(2):130–139
Scuffham P, Chaplin S, Legood R (2003) Incidence and costs of unintentional falls in older people in the United Kingdom. J Epidemiol Community Health 57(9):740–744
Sherrington C, Tiedemann A, Fairhall N, Close JC, Lord SR (2011) Exercise to prevent falls in older adults: an updated meta-analysis and best practice recommendations. N S W Public Health Bull 22(3–4):78–83
Sherrington C, Whitney JC, Lord SR, Herbert RD, Cumming RG, Close JCT (2008) Effective exercise for the prevention of falls: a systematic review and meta-analysis. J Am Geriatr Soc 56(12):2234–2243
Shumway-Cook A, Silver IF, LeMier M, York S, Cummings P, Koepsell TD (2007) Effectiveness of a community-based multifactorial intervention on falls and fall risk factors in community-living older adults: a randomized, controlled trial. J Gerontol A Biol Sci Med Sci 62(12):1420–1427
Skelton D, Dinan S, Campbell M, Rutherford O (2005) Tailored group exercise (Falls Management Exercise—FaME) reduces falls in community-dwelling older frequent fallers (an RCT). Age Ageing 34(6):636–639
Society AG, Society BG (2011) Summary of the updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc. doi:10.1111/j.1532-5415.2010.03234.x
Steinberg M, Cartwright C, Peel N, Williams G (2000) A sustainable programme to prevent falls and near falls in community dwelling older people: results of a randomised trial. J Epidemiol Community Health 54(3):227–232
Suzuki T, Kim H, Yoshida H, Ishizaki T (2004) Randomized controlled trial of exercise intervention for the prevention of falls in community-dwelling elderly Japanese women. J Bone Miner Metab 22(6):602–611
Thomas S, Mackintosh S, Halbert J (2010) Does the ‘Otago exercise programme’ reduce mortality and falls in older adults?: a systematic review and meta-analysis. Age Ageing 39(6):681–687
Tinetti ME, Baker DI, McAvay G, Claus EB, Garrett P, Gottschalk M, Koch ML, Trainor K, Horwitz RI (1994) A multifactorial intervention to reduce the risk of falling among elderly people living in the community. N Engl J Med 331(13):821–827
Tinetti ME, Williams CS (1997) Falls, injuries due to falls, and the risk of admission to a nursing home. N Engl J Med 337(18):1279–1284
Visek AJ, Olson EA, DiPietro L (2011) Factors predicting adherence to 9 months of supervised exercise in healthy older women. J Phys Act Health 8(1):104–110
Weerdesteyn V, Rijken H, Geurts AC, Smits-Engelsman BC, Mulder T, Duysens J (2006) A five-week exercise program can reduce falls and improve obstacle avoidance in the elderly. Gerontology 52(3):131–141
Wolf SL, Barnhart HX, Kutner NG, McNeely E, Coogler C, Xu T (1996) Reducing frailty and falls in older persons: an investigation of tai chi and computerized balance training. Atlanta FICSIT Group. Frailty and injuries: cooperative studies of intervention techniques. J Am Geriatr Soc 44(5):489–497
Woo J, Hong A, Lau E, Lynn H (2007) A randomised controlled trial of tai chi and resistance exercise on bone health, muscle strength and balance in community-living elderly people. Age Ageing 36(3):262–268
Wu G, Keyes L, Callas P, Ren X, Bookchin B (2010) Comparison of telecommunication, community, and home-based tai chi exercise programs on compliance and effectiveness in elders at risk for falls. Arch Phys Med Rehabil 91(6):849–856
Yamada M, Tanaka B, Nagai K, Aoyama T, Ichihashi N (2010) Trail-walking exercise and fall risk factors in community-dwelling older adults: preliminary results of a randomized controlled trial. J Am Geriatr Soc 58(10):1946–1951
Acknowledgments
The first author wishes to acknowledge Dr. John Nelson and Dr. Pepijn Van De Ven, University of Limerick, for their supervision and guidance. The first author is funded via Enhanced Complete Ambient Assisted Living Experiment, a project funded by the European Commission under the Ambient Assisted Living Joint Programme.
Conflict of interest
The authors have no conflict of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Power, V., Clifford, A.M. Characteristics of optimum falls prevention exercise programmes for community-dwelling older adults using the FITT principle. Eur Rev Aging Phys Act 10, 95–106 (2013). https://doi.org/10.1007/s11556-012-0108-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11556-012-0108-2