
Abstract
Purpose
Pulmonary artery sarcomas (PAS) are rare malignant tumours that originate from the intimal layer of the pulmonary artery, occur in middle age and have a poor prognosis. In planning appropriate treatment, malignant disease should be suspected whenever there are specific clinical and radiological manifestations, in order to establish the differential diagnosis with acute pulmonary embolism or chronic thromboembolic pulmonary hypertension, with which this malignancy is most commonly confused.
Materials and methods
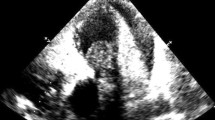
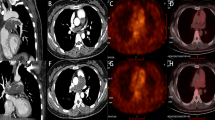
Between 2008 and 2012, we managed four adult patients with a nonspecific clinical presentation who, at the conclusion of the diagnostic process, were found to be affected by PAS. Because of the initial suspicion of pulmonary embolism, all patients underwent chest radiograph, lung perfusion scintigraphy, trans-oesophageal echocardiography, and computed tomography (CT) angiography of the chest. Then, because of the peculiar CT findings and lack of response to anticoagulation therapy, a clinical suspicion of PAS was considered and all patients underwent positron-emission tomography (PET)-CT, and one patient also magnetic resonance imaging (MRI) of the chest. Subsequently, all patients underwent thromboendoarterectomy with histological investigation of the surgical specimen, which confirmed the clinical and radiological suspicion of PAS.
Results
CT is the technique that enabled the first step in the differential diagnosis between PAS and pulmonary embolism. The CT characteristics suggestive of PAS included the particular filling defect occupying the entire lumen of the pulmonary trunk with increase in diameter of the involved vessel and patchy and delayed contrast enhancement at CT angiography, more evident in the venous phase. PET-CT was used to differentiate between PAS and pulmonary embolism on the basis of the intensity of increased radiopharmaceutical uptake. MRI was used in one case of equivocal results on PET-CT, to improve tissue characterisation of the lesions and differentiation between the thrombotic and neoplastic components.
Conclusions
The radiologist is usually the first to raise a suspicion of PAS in patients with severe dyspnoea and filling defect in the pulmonary artery, unresponsive to anticoagulation therapy. Combining CT and PET-CT proved to be extremely useful in assessing patients with suspected PAS. Early diagnosis with the help of integrated imaging remains today the main direction to pursue in order to obtain improvements in prognosis.
Riassunto
Obiettivo
I sarcomi dell’arteria polmonare (SAP) sono rari tumori maligni che originano dallo strato intimale dell’arteria polmonare, insorgono nell’età media e hanno una prognosi sfavorevole. Per impostare l’approccio terapeutico adeguato è opportuno sospettare la patologia tumorale qualora si presentino peculiari manifestazioni radiologiche e cliniche, al fine di porre la diagnosi differenziale con il quadro di embolia polmonare acuta piuttosto che di ipertensione polmonare cronica tromboembolica, con le quali tale patologia neoplastica è più comunemente confusa.
Materiali e metodi
Tra il 2008 ed il 2012 sono giunti alla nostra osservazione 4 pazienti adulti, con quadro clinico non specifico che al termine dell’iter diagnostico sono risultati affetti da SAP. Tutti i pazienti, per il sospetto iniziale di embolia polmonare, hanno eseguito una radiografia del torace, una scintigrafia polmonare perfusionale, un’ecocardiografia trans-esofagea, e una angio-tomografia computerizzata (TC) torace. In seguito alle peculiari caratteristiche TC associate alla mancata risposta alla terapia anticoagulante, nel sospetto clinico di SAP, è stata effettuata una tomografia ad emissione di positroni (PET)-TC ed in un caso anche una risonanza magnetica (RM) toracica. In seguito tutti i pazienti sono stati sottoposti a tromboendoarteriectomia con indagine istologica del pezzo operatorio che ha confermato il sospetto clinico-radiologico di SAP.
Risultati
La TC è la metodica che ha permesso di effettuare il primo step nella diagnosi differenziale tra SAP ed embolia polmonare. Le caratteristiche suggestive per SAP includevano il particolare difetto di riempimento occupante l’intero lume del tronco polmonare con aumento di diametro del vaso coinvolto e il contrast enhancement disomogeneo e ritardato alla angio-TC, ancora più evidente in fase venosa. La PET-TC è stata impiegata per confermare il sospetto di SAP e distinguere tra SAP ed embolia polmonare sulla base dell’ipercaptazione del radiofarmaco della componente neoplastica. La RM è stata utilizzata in un caso con PET-TC dubbia per una migliore caratterizzazione tissutale della lesione e per meglio differenziare la componente trombotica da quella neoplastica.
Conclusioni
Il radiologo è in genere il primo a potere porre il sospetto di SAP in pazienti con grave dispnea e difetto di riempimento nell’arteria polmonare non responsivi alla terapia anticoagulante. La combinazione TC e PET-TC si è rivelata di estrema utilità nella valutazione dei pazienti con sospetto SAP. La diagnosi precoce mediante imaging integrato rimane ancora al giorno d’oggi la via principale da perseguire per ottenere miglioramenti in termini prognostici.
Similar content being viewed by others

References/Bibliografia
Blackmon SH, Reardon MJ (2010) Pulmonary artery sarcoma. Methodist Debakey Cardiovasc J 6:38–43
Huo L, Lai S, Gladish G et al (2005) Pulmonary artery angiosarcoma: a clinicopathologic and radiological correlation. Ann Diagn Pathol 9:209–214
Burke AP, Virmani R (1993) Sarcomas of the great vessels. A clinicopathologic study. Cancer 71:1761–1773
Cox JE, Chiles C, Aquino SL et al (1997) Pulmonary artery sarcomas: a review of clinical and radiologic features. J Comput Assist Tomogr 21:750–755
Simpson WL, Mendelson DS (2000) Pulmonary artery and aortic sarcomas: cross-sectional imaging. J Thorac Imaging 15:290–294
Pandit SA, Fiedler PN, Westcott JL (2005) Primary angiosarcoma of the lung. Annals Diagn Pathol 9:302–304
Scheffel H, Stolzmann P, Plass A et al (2008) Primary intimal pulmonary artery sarcoma: a diagnostic challenge. J Thorac Cardiovasc Surg 135:949–950
De Luca F, Modolon C, Buia F et al (2012) Densitometric CT evaluation of acute and chronic thromboembolic filling defects of the pulmonary arteries before and after contrast injection. Radiol Med 117:979–991
Ito K, Kubota K, Morooka M (2009) Diagnostic usefulness of 18F-FDG PET/CT in the differentiation of pulmonary artery sarcoma and pulmonary embolism. Ann Nucl Med 23:671–676
Chong S, Kim TS, Kim BT (2007) Pulmonary artery sarcoma mimicking pulmonary thromboembolism: integrated FDG PET/CT. AJR Am J Roentgenol 188:1691–1693
Kauczor HU, Schwickert HC, Mayer E et al (1994) Pulmonary artery sarcoma mimicking chronic thromboembolic disease: computed tomography and magnetic resonance imaging findings. Cardiovasc Intervent Radiol 17:185–189
Kacl GM, Bruder E, Pfammatter T (1998) Primary angiosarcoma of the pulmonary arteries: dynamic contrastenhanced MRI. J Comput Assist Tomogr 22:687–691
Rafal RB, Nichols JN, Markisz JA (1995) Pulmonary artery sarcoma: diagnosis and postoperative follow-up with gadolinium-diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging. Mayo Clin Proc 70:173–176
Kojima K, Okamoto I, Ushijima S et al (2003) Successful treatment of primary pulmonary angiosarcoma. Chest 124:2397–2400
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Attinà, D., Niro, F., Tchouanté, P. et al. Pulmonary artery intimal sarcoma. Problems in the differential diagnosis. Radiol med 118, 1259–1268 (2013). https://doi.org/10.1007/s11547-013-0943-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-013-0943-x
Keywords
- Pulmonary artery sarcoma
- Differential diagnosis
- Computed tomography
- Magnetic resonance imaging
- Positron emission tomography