
Abstract
Purpose
Men with prolactin-secreting tumors usually harbor macroadenomas. The degree of pituitary dysfunction may vary among different adenoma size subgroups, as is recovery after treatment. Our study purpose was to characterize hypopituitarism and recovery after treatment in men with macroprolactinomas.
Methods
A retrospective study, including a consecutive group of 81 men with pituitary macroadenomas (≥10 mm) and hyperprolactinemia (>7×ULN). Patients were divided into three categories according to adenoma size at presentation: 10–19 mm (group A), 20–39 mm (group B), and ≥40 mm (group C). We compared total testosterone, gonadotropins, cortisol, thyroid hormones and hemoglobin levels at presentation and after treatment.
Results
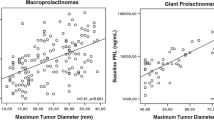
Eighty-one patients were included; 24, 31 and 26 patients in groups A, B and C, respectively. Pretreatment hypogonadism prevalence was 75.0, 93.5 and 90.9 % (p = 0.046; A vs B and C), central hypocortisolism − 0, 6.9 and 33.3 % (p = 0.005), and central hypothyroidism − 6.7, 17.9 and 26.1 % (NS) in groups A, B and C, respectively. Only 26.7 % of all patients presented with hypocortisolism and/or hypothyroidism (42.9 % in group C). Anemia (Hb < 13.5 g %) was detected in 31.3, 57.1 and 80.0 % in groups A, B and C, respectively (p = 0.04). Larger adenoma diameter correlated strongly with lower FT4 levels following treatment (r = −0.42, p = 0.043).
Conclusions
Macroprolactinomas in men caused partial hypopituitarism, affecting testosterone in all adenoma size groups and cortisol more in patients with larger adenomas. However, most of the men did not have pituitary hormones affected, beside testosterone. Most patients recovered central hypocortisolism but not hypothyroidism following treatment.



Similar content being viewed by others


References
Grossman A, Besser GM (1985) Prolactinomas. Br Med J (Clin Res Ed) 290:182–184
Colao A, Di Sarno A, Cappabianca P, Briganti F, Pivonello R, Somma CD, Faggiano A, Biondi B, Lombardi G (2003) Gender differences in the prevalence, clinical features and response to cabergoline in hyperprolactinemia. Eur J Endocrinol 148:325–331
Delgrange E, Trouillas J, Maiter D, Donckier J, Tourniaire J (1997) Sex-related difference in the growth of prolactinomas: a clinical and proliferation marker study. J Clin Endocrinol Metab 82:2102–2107
Colao A, Vitale G, Cappabianca P, Briganti F, Ciccarelli A, De Rosa M, Zarrilli S, Lombardi G (2004) Outcome of cabergoline treatment in men with prolactinoma: effects of a 24-month treatment on prolactin levels, tumor mass, recovery of pituitary function, and semen analysis. J Clin Endocrinol Metab 89:1704–1711
Sibal L, Ugwu P, Kendall-Taylor P, Ball SG, James RA, Pearce SH, Hall K, Quinton R (2002) Medical therapy of macroprolactinomas in males: I. prevalence of hypopituitarism at diagnosis. II. Proportion of cases exhibiting recovery of pituitary function. Pituitary 5:243–246
Karavitaki N, Dobrescu R, Byrne JV, Grossman AB, Wass JA (2013) Does hypopituitarism recover when macroprolactinomas are treated with cabergoline? Clin Endocrinol (Oxf) 79:217–223
Iglesias P, Bernal C, Villabona C, Castro JC, Arrieta F, Díez JJ (2012) Prolactinomas in men: a multicentre and retrospective analysis of treatment outcome. Clin Endocrinol (Oxf) 77:281–287
Shimon I, Benbassat C, Hadani M (2007) Effectiveness of long-term cabergoline treatment for giant prolactinoma: study of 12 men. Eur J Endocrinol 156:225–231
Nomikos P, Ladar C, Fahlbusch R, Buchfelder M (2004) Impact of primary surgery on pituitary function in patients with non-functioning pituitary adenomas—a study on 721 patients. Acta Neurochir (Wien) 146:27–35
Arafah BM, Prunty D, Ybarra J, Hlavin ML, Selman WR (2000) The dominant role of increased intrasellar pressure in the pathogenesis of hypopituitarism, hyperprolactinemia, and headaches in patients with pituitary adenomas. J Clin Endocrinol Metab 85:1789–1793
Vroonen L, Jaffrain-Rea ML, Petrossians P, Tamagno G, Chanson P, Vilar L, Borson-Chazot F, Naves LA, Brue T, Gatta B, Delemer B, Ciccarelli E, Beck-Peccoz P, Caron P, Daly AF, Beckers A (2012) Prolactinomas resistant to standard doses of cabergoline: a multicenter study of 92 patients. Eur J Endocrinol 167:651–662
Comtois R, Beauregard H, Somma M, Serri O, Aris-Jilwan N, Hardy J (1991) The clinical and endocrine outcome to trans-sphenoidal microsurgery of nonsecreting pituitary adenomas. Cancer 68:860–866
Wichers-Rother M, Hoven S, Kristof RA, Bliesener N, Stoffel-Wagner B (2004) Non-functioning pituitary adenomas: endocrinological and clinical outcome after transsphenoidal and transcranial surgery. Exp Clin Endocrinol Diabetes 112:323–327
Dekkers OM, Pereira AM, Roelfsema F, Voormolen JH, Neelis KJ, Schroijen MA, Smit JW, Romijn JA (2006) Observation alone after transsphenoidal surgery for nonfunctioning pituitary macroadenoma. J Clin Endocrinol Metab 91:1796–1801
Ciccarelli A, Guerra E, De Rosa M, Milone F, Zarrilli S, Lombardi G, Colao A (2005) PRL secreting adenomas in male patients. Pituitary 8:39–42
Shimon I, Benbassat C (2013) Male prolactinomas presenting with normal testosterone levels. Pituitary
Matsumoto AM, Bremner WJ (2011) Testicular disorders. In: Melmed S, Polonsky KS, Larsen PR, Kronenberg HM (eds) Williams textbook of endocrinology, 12th edn. Elsevier, Philadelphia, p 746
Pinzone JJ, Katznelson L, Danila DC, Pauler DK, Miller CS, Klibanski A (2000) Primary medical therapy of micro- and macroprolactinomas in men. J Clin Endocrinol Metab 85:3053–3057
Iglesias P, Castro JC, Díez JJ (2011) Clinical significance of anaemia associated with prolactin-secreting pituitary tumours in men. Int J Clin Pract 65:669–673
Mazziotti G, Porcelli T, Mormando M, De Menis E, Bianchi A, Mejia C, Mancini T, De Marinis L, Giustina A (2011) Vertebral fractures in males with prolactinoma. Endocrine 39:288–293
Anagnostis P, Adamidou F, Polyzos SA, Efstathiadou Z, Karathanassi E, Kita M (2012) Long term follow-up of patients with prolactinomas and outcome of dopamine agonist withdrawal: a single center experience. Pituitary 15:25–29
Acknowledgements
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tirosh, A., Benbassat, C., Lifshitz, A. et al. Hypopituitarism patterns and prevalence among men with macroprolactinomas. Pituitary 18, 108–115 (2015). https://doi.org/10.1007/s11102-014-0563-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-014-0563-z