
Abstract
Purpose
To probe the suitability of a dry-powder oxytocin formulation containing a carrier (μco™; SNBL, Ltd.) for intranasal (IN) administration to treat post-partum hemorrhage in the developing world. Specifically, to investigate (1) whether IN administration can achieve rapid systemic absorption in cynomolgus monkeys, and (2) whether the formulation exhibits sufficient physical and chemical stability. This study was conducted to support Merck for Mothers, Merck’s 10-year global initiative to end preventable maternal deaths.
Methods
A partial-crossover pharmacokinetic (PK) study in cynomolgus monkeys (n = 6) was utilized to compare in vivo absorption of dry-powder IN oxytocin at three dose levels against an IM injection of an aqueous oxytocin formulation. Particle size distribution, delivered dose and chemical assay were monitored over a 12 month stability study.
Results
IN administration of oxytocin resulted in short (5 min) Tmax and good dose linearity in AUC and Cmax over the dose range tested (10–80 IU per animal). The relative bioavailability (BA) of IN oxytocin to IM injection was approximately 12%. The 80 IU formulation exhibited good physical stability and consistent dosing. After 12 months at 30°C/65%RH, pouched samples retained 86.0% of their original assay value.
Conclusions
The PK and stability data suggests that IN administration of oxytocin formulated in the μco™ carrier may represent a viable option for rapid systemic absorption in humans and a product compatible with resource-scarce regions.





Similar content being viewed by others

Abbreviations
- AUC:
-
Area under the curve
- BA:
-
Bioavailability
- Cmax :
-
Maximum plasma concentration of drug
- Dv10:
-
The diameter of particles where 10% of the population by volume lies below this value
- Dv50:
-
The diameter of particles where half of the population by volume lies below this value
- Dv90:
-
The diameter of particles where 90% of the population by volume lies below this value
- IM:
-
Intramuscular
- IN:
-
Intranasal
- IU:
-
International units
- PK:
-
Pharmacokinetic
- PPH:
-
Postpartum hemorrhage
- RH:
-
Relative humidity
- SD:
-
Standard deviation
- Tmax :
-
Time to maximum plasma concentration of drug
References
WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Trends in maternal mortality: 1990 to 2015. Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division, 2015.
The United Nations. We can end poverty: Millenium development goals and beyond 2015. http://www.un.org/millenniumgoals/maternal.shtml.
Carroli G, Cuesta C, Abalos E, Gulmezoglu AM. Epidemiology of postpartum haemorrhage: a systematic review. Best Pract Res. 2008;22:999–1012.
Mousaand HA, Alfirevic Z. Treatment for primary postpartum haemorrhage. The Cochrane database of systematic reviews:CD003249 (2003).
Dina Abbas JD, Winikoff B. Proposal for the inclusion of misoprostol in the WHO model list of essential medicines, 20th Expert Committee on the Selection and Use of Essential Medicines Geneva, 2015, 2015.
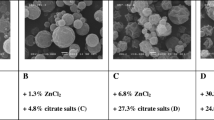
Avanti C, Amorij JP, Setyaningsih D, Hawe A, Jiskoot W, Visser J, et al. A new strategy to stabilize oxytocin in aqueous solutions: I. The effects of divalent metal ions and citrate buffer. AAPS J. 2011;13:284–90.
Avanti C, Permentier HP, Dam A, Poole R, Jiskoot W, Frijlink HW, et al. A new strategy to stabilize oxytocin in aqueous solutions: II. Suppression of cysteine-mediated intermolecular reactions by a combination of divalent metal ions and citrate. Mol Pharm. 2012;9:554–62.
Fabio K, Curley K, Guarneri J, Adamo B, Laurenzi B, Grant M, Offord R, Kraft K, Leone-Bay A. Heat-stable dry powder oxytocin formulations for delivery by oral inhalation. AAPS PharmSciTech (2015).
Prankerd RJ, Nguyen TH, Ibrahim JP, Bischof RJ, Nassta GC, Olerile LD, et al. Pulmonary delivery of an ultra-fine oxytocin dry powder formulation: potential for treatment of postpartum haemorrhage in developing countries. PLoS One. 2013;8, e82965.
Dal Monte O, Noble PL, Turchi J, Cummins A, Averbeck BB. CSF and blood oxytocin concentration changes following intranasal delivery in macaque. PLoS One. 2014;9, e103677.
Suman JD. Nasal drug delivery. Expert Opin Biol Ther. 2003;3:519–23.
Harkema JR. Comparative aspects of nasal airway anatomy: relevance to inhalation toxicology. Toxicol Pathol. 1991;19:321–36.
O’Haganand DT, Illum L. Absorption of peptides and proteins from the respiratory tract and the potential for development of locally administered vaccine. Crit Rev Ther Drug Carrier Syst. 1990;7:35–97.
Ozsoy Y, Gungor S, Cevher E. Nasal delivery of high molecular weight drugs. Molecules (Basel, Switzerland). 2009;14:3754–79.
De Groot AN, Vree TB, Hekster YA, Pesman GJ, Sweep FC, Van Dongen PJ, et al. Bioavailability and pharmacokinetics of sublingual oxytocin in male volunteers. J Pharm Pharmacol. 1995;47:571–5.
ACKNOWLEDGMENTS AND DISCLOSURES
The authors would like to thank Pastorus Pharma, LLC owner of the license for the dry-powder oxytocin formulation for making it available for Merck-for-Mothers study and sharing pharmacokinetic data of an independent study involving intranasal oxytocin. This research was supported by funding from Merck & Co., Inc., Kenilworth, NJ through its Merck for Mothers program, a $500 Million, 10-year initiative to reducing maternal mortality.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Milewski, M., Goodey, A., Lee, D. et al. Rapid Absorption of Dry-Powder Intranasal Oxytocin. Pharm Res 33, 1936–1944 (2016). https://doi.org/10.1007/s11095-016-1929-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11095-016-1929-x