
Abstract
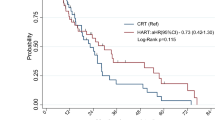
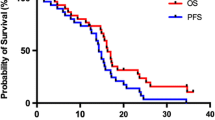
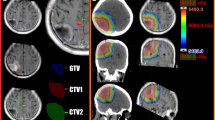
To compare progression-free (PFS) and overall survival (OS) in patients treated in two consecutive phase II trials of hypofractionated-intensity modulated radiotherapy (hypo-IMRT) and temozolomide (TMZ) with or without bevacizumab (BEV). Patients with newly diagnosed glioblastoma multiforme (GBM) after biopsy or resection were enrolled on a clinical trial with hypo-IMRT and TMZ (hypo-IMRT/TMZ alone) from 2008 to 2010, or in the second protocol with the same hypo-IMRT and TMZ plus BEV (hypo-IMRT/TMZ/BEV) from 2010 to 2013. All patients received postoperative hypo-IMRT to the surgical cavity and residual tumor plus margin to a total dose of 60 Gy and to the T2 abnormality with margin to 30 Gy, both in ten fractions. Concurrent TMZ (75 mg/m2/day) was given to all patients for 28 consecutive days followed by adjuvant TMZ (150–200 mg/m2/day). Patients enrolled on the hypo-IMRT/TMZ/BEV trial received concurrent and adjuvant BEV (10 mg/kg) on days 1 and 15 of each 28-day cycle. Hazard ratios of PFS and OS were compared between trials in a Cox proportional hazards model. Twenty-six patients were enrolled on the hypo-IMRT/TMZ alone trial and 30 patients on the hypo-IMRT/TMZ/BEV trial. Median follow-up was 13.9 and 14.7 months, respectively. Median PFS was 3.4 months longer with hypo-IMRT/TMZ/BEV but the difference was not statistically significant (12.8 vs. 9.4 months, p = 0.58). Median (OS) was 16.3 months for both trials. The addition of BEV to TMZ and hypo-IMRT did not improve OS for patients with GBM in two phase II trials with small patient numbers; PFS was longer with BEV, but the difference was not statistically significant.


Similar content being viewed by others
References
Stupp R, Mason WP, van den Bent MJ et al (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352:987–996
Stupp R, Hegi ME, Mason WP et al (2009) Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 10:459–466
Chen C, Damek D, Gaspar LE et al (2011) Phase I trial of hypofractionated intensity-modulated radiotherapy with temozolomide chemotherapy for patients with newly diagnosed glioblastoma multiforme. Int J Radiat Oncol Biol Phys 81:1066–1074
Reddy K, Damek D, Gaspar LE et al (2012) Phase II trial of hypofractionated IMRT with temozolomide for patients with newly diagnosed glioblastoma multiforme. Int J Radiat Oncol Biol Phys 84:655–660
Reddy K, Gaspar LE, Kavanagh BD et al (2014) Hypofractionated intensity-modulated radiotherapy with temozolomide chemotherapy may alter the patterns of failure in patients with glioblastoma multiforme. J Med Imaging Radiat Oncol 58:714–721
Birner P, Piribauer M, Fischer I et al (2003) Vascular patterns in glioblastoma influence clinical outcome and associate with variable expression of angiogenic proteins: evidence for distinct angiogenic subtypes. Brain Pathol 13:133–143
Godard S, Getz G, Delorenzi M et al (2003) Classification of human astrocytic gliomas on the basis of gene expression: a correlated group of genes with angiogenic activity emerges as a strong predictor of subtypes. Cancer Res 63:6613–6625
Stefanik DF, Fellows WK, Rizkalla LR et al (2001) Monoclonal antibodies to vascular endothelial growth factor (VEGF) and the VEGF receptor, FLT-1, inhibit the growth of C6 glioma in a mouse xenograft. J Neurooncol 55:91–100
Kim KJ, Li B, Winer J et al (1993) Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo. Nature 362:841–844
Kreisl TN, Kim L, Moore K et al (2009) Phase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastoma. J Clin Oncol 27:740–745
Vredenburgh JJ, Desjardins A, Herndon JE et al (2007) Bevacizumab plus irinotecan in recurrent glioblastoma multiforme. J Clin Oncol 25:4722–4729
Friedman HS, Prados MD, Wen PY et al (2009) Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol 27:4733–4740
Lai A, Filka E, McGibbon B et al (2008) Phase II pilot study of bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly diagnosed glioblastoma multiforme: interim analysis of safety and tolerability. Int J Radiat Oncol Biol Phys 71:1372–1380
Gutin PH, Iwamoto FM, Beal K et al (2009) Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int J Radiat Oncol Biol Phys 75:156–163
Ney D, Carlson JA, Damek DM et al (2015) Phase II trial of hypofractionated intensity-modulated radiation therapy combined with temozolomide and bevacizumab for patients with newly diagnosed glioblastoma. J Neurooncol 122:135–143
Gonzalez J, Kumar AJ, Conrad CA et al (2007) Effect of bevacizumab on radiation necrosis of the brain. Int J Radiat Oncol Biol Phys 67:323–326
Torcuator R, Zuniga R, Mohan YS et al (2009) Initial experience with bevacizumab treatment for biopsy confirmed cerebral radiation necrosis. J Neurooncol 94:63–68
Wong ET, Huberman M, Lu XQ et al (2008) Bevacizumab reverses cerebral radiation necrosis. J Clin Oncol 26:5649–5650
Salmaggi A, Eoli M, Frigerio S et al (2003) Intracavitary VEGF, bFGF, IL-8, IL-12 levels in primary and recurrent malignant glioma. J Neurooncol 62:297–303
Lamszus K, Ulbricht U, Matschke J et al (2003) Levels of soluble vascular endothelial growth factor (VEGF) receptor 1 in astrocytic tumors and its relation to malignancy, vascularity, and VEGF-A. Clin Cancer Res 9:1399–1405
Coderre JA, Morris GM, Micca PL et al (2006) Late effects of radiation on the central nervous system: role of vascular endothelial damage and glial stem cell survival. Radiat Res 166:495–503
Chinot OL, Wick W, Mason W et al (2014) Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N Engl J Med 370:709–722
Gilbert MR, Dignam JJ, Armstrong TS et al (2014) A randomized trial of bevacizumab for newly diagnosed glioblastoma. N Engl J Med 370:699–708
Minniti G, Clarke E, Lanzetta G et al (2011) Stereotactic radiosurgery for brain metastases: analysis of outcome and risk of brain radionecrosis. Radiat Oncol 6:48
Blonigen BJ, Steinmetz RD, Levin L et al (2010) Irradiated volume as a predictor of brain radionecrosis after linear accelerator stereotactic radiosurgery. Int J Radiat Oncol Biol Phys 77:996–1001
Omuro A, Beal K, Gutin P et al (2014) Phase II study of bevacizumab, temozolomide, and hypofractionated stereotactic radiotherapy for newly diagnosed glioblastoma. Clin Cancer Res 20:5023–5031
Jain RK (2005) Normalization of tumor vasculature: an emerging concept in antiangiogenic therapy. Science 307:58–62
Jeyaretna DS, Curry WT Jr, Batchelor TT et al (2011) Exacerbation of cerebral radiation necrosis by bevacizumab. J Clin Oncol 29:e159–e162
Conflict of interest
The authors report no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Carlson, J.A., Reddy, K., Gaspar, L.E. et al. Hypofractionated-intensity modulated radiotherapy (hypo-IMRT) and temozolomide (TMZ) with or without bevacizumab (BEV) for newly diagnosed glioblastoma multiforme (GBM): a comparison of two prospective phase II trials. J Neurooncol 123, 251–257 (2015). https://doi.org/10.1007/s11060-015-1791-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-015-1791-4