
Abstract
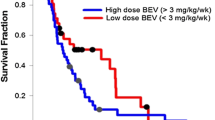
Bevacizumab (BEV, Avastin®) produces durable objective radiological responses of 20–26 %, median response durations of 16–18 weeks, and median overall survival (mOS) of 31–40 weeks. While the use of BEV is well-established, the lack of dose–response studies in glioblastoma (GBM) patients raises the question whether current dosing practice is optimal. As a result of differing approaches to BEV dosing that ranged from the FDA approved package insert dose of 10 mg/kg every 2 weeks to 7.5 mg/kg every 3–4 weeks, among physicians within Northern California Kaiser Permanente hospitals over 4+ years, we did an IRB-approved retrospective analysis of patients seen in Northern California Kaiser Permanente facilities and treated with BEV. Between September 1, 2008 and August 31, 2013, 181 patients received BEV for tumor progression/recurrence starting 2.6 weeks after completion of chemoradiation. The integrated BEV administered dose-week (AUCBEV) for all patients had a median AUCBEV of 3.6 mg·wk/kg). Maximum likelihood analysis found patients over 65 years did worse than younger patients (p = 0.004), women lived longer (p = 0.002), and patients treated below the AUCBEV did better than those treated above the median AUCBEV (p = 0.003). mOS for BEV starting 1 month after chemoradiation was 45 versus 68 weeks (p = 0.012) and BEV starting 3 months after chemoradiation was 40 versus 74 weeks (p = 0.0085). Dosing BEV at half the standard dose for progressive/recurrent GBM was at least equivalent to or, maybe better than standard dosing. Unexplained was the observation that females had longer OS with BEV than males.



Similar content being viewed by others


References
Friedman HS, Prados MD, Wen PY et al (2009) Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol 27(28):4733–4740
Cohen MH, Shen YL, Keegan P, Pazdur R (2009) FDA drug approval summary: Bevacizumab (Avastin®) as treatment of recurrent Glioblastoma Multiforme. Oncologist 14(11):1131–1138
Desjardins A, Reardon DA, Herndon JE II et al (2008) Bevacizumab plus irinotecan in recurrent WHO grade 3 malignant gliomas. Clin Cancer Res 14(21):7068–7073
Kreisl TN, Kim L, Moore K et al (2009) Phase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastoma. J Clin Oncol 27(5):740–745
Gonzalez J, Kumar AJ, Conrad CA, Levin VA (2007) Effect of bevacizumab on radiation necrosis of the brain. Int J Radiat Oncol Biol Phys 67(2):323–326
Levin VA, Bidaut L, Hou P et al (2011) Randomized double-blind placebo-controlled trial of bevacizumab therapy for radiation necrosis of the central nervous system. Int J Radiat Oncol Biol Phys 79(5):1487–1495
Wong ET, Huberman M, Lu XQ, Mahadevan A (2008) Bevacizumab Reverses Cerebral Radiation Necrosis. J Clin Oncol 26:5649–5650
Liu AK, Macy ME, Foreman NK (2009) Bevacizumab as therapy for radiation necrosis in four children with pontine gliomas. Int J Radiat Oncol Biol Phys 75(4):1148–1154
Torcuator R, Zuniga R, Mohan YS et al (2009) Initial experience with bevacizumab treatment for biopsy confirmed cerebral radiation necrosis. J Neurooncol 94(1):63–68
Lubelski D, Abdullah K, Weil R, Marko N (2013) Bevacizumab for radiation necrosis following treatment of high grade glioma: a systematic review of the literature. J Neurooncol 115(3):317–322
Lu JF, Bruno R, Eppler S, Novotny W, Lum B, Gaudreault J (2008) Clinical pharmacokinetics of bevacizumab in patients with solid tumors. Cancer Chemother Pharmacol 62(5):779–786
Wick W, Weller M, van den Bent M, Stupp R (2010) Bevacizumab and recurrent malignant gliomas: a European perspective. J Clin Oncol. 28(12):e188–e189 (author reply e190-182)
Levin VA, Edwards MS, Wright DC et al (1980) Modified procarbazine, CCNU, and vincristine (PCV 3) combination chemotherapy in the treatment of malignant brain tumors. Cancer Treat Rep 64(2–3):237–244
Kaplan EL, Meier P (1958) Nonparametric estimates from incomplete observations. J Am Statist Assoc 53:457–481
Mantel N (1966) Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 50(3):163–170
Gehan EA (1965) A generalized Wilcoxon test for comparing arbitrarily singly-censored samples. Biometrika 52:203–223
Hoffman WF, Levin VA, Wilson CB (1979) Evaluation of malignant glioma patients during the postirradiation period. J Neurosurg 50(5):624–628
Brandes AA, Tosoni A, Spagnolli F et al (2008) Disease progression or pseudoprogression after concomitant radiochemotherapy treatment: pitfalls in neurooncology. Neuro Oncol. 10(3):361–367
Brandsma D, Stalpers L, Taal W, Sminia P, van den Bent MJ (2008) Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol 9(5):453–461
Chamberlain MC (2008) Pseudoprogression in glioblastoma. J Clin Oncol 26(26):4359 author reply 4359–4360
Brandsma D, van den Bent MJ (2009) Pseudoprogression and pseudoresponse in the treatment of gliomas. Curr Opin Neurol 22(6):633–638
Chaskis C, Neyns B, Michotte A, de Ridder M, Everaert H (2009) Pseudoprogression after radiotherapy with concurrent temozolomide for high-grade glioma: clinical observations and working recommendations. Surg Neurol 72(4):423–428
Clarke JL, Chang S (2009) Pseudoprogression and pseudoresponse: challenges in brain tumor imaging. Curr Neurol Neurosci Rep 9(3):241–246
Taal W, Oosterkamp HM, Walenkamp AM et al (2014) Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): a randomised controlled phase 2 trial. Lancet Oncol 15(9):943–953
Piccioni DE, Selfridge J, Mody RR et al (2014) Deferred use of bevacizumab for recurrent glioblastoma is not associated with diminished efficacy. Neuro Oncol 16(6):815–822
Raizer JJ, Grimm S, Chamberlain MC et al (2010) A phase 2 trial of single-agent bevacizumab given in an every-3-week schedule for patients with recurrent high-grade gliomas. Cancer 116(22):5297–5305
Wong ET, Gautam S, Malchow C, Lun M, Pan E, Brem S (2011) Bevacizumab for recurrent glioblastoma multiforme: a meta-analysis. J Natl Compr Canc Netw 9(4):403–407
Rodriguez MA, DeJesus AY, Cheng L (2014) Use of chemotherapy within the last 14 days of life in patients treated at a comprehensive cancer center. JAMA Intern Med 174(6):989–991
Funding
Internal Kaiser Permanente funding.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Levin, V.A., Mendelssohn, N.D., Chan, J. et al. Impact of bevacizumab administered dose on overall survival of patients with progressive glioblastoma. J Neurooncol 122, 145–150 (2015). https://doi.org/10.1007/s11060-014-1693-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-014-1693-x