
Abstract
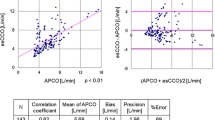
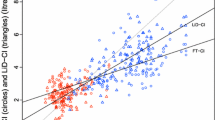
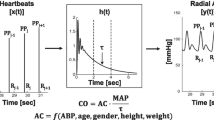
Estimated continuous cardiac output (esCCO), a noninvasive technique for continuously measuring cardiac output (CO), is based on modified pulse wave transit time, which in turn is determined by pulse oximetry and electrocardiography. However, its trending ability has never been evaluated in patients undergoing non-cardiac surgery. Therefore, this study examined esCCO’s ability to detect the exact changes in CO, compared with currently available arterial waveform analysis methods, in patients undergoing kidney transplantation. CO was measured using an esCCO system and arterial pressure-based CO (APCO), and compared with a corresponding intermittent bolus thermodilution CO (ICO) method. Percentage error and statistical methods, including concordance analysis and polar plot analysis, were used to analyze results from 15 adult patients. The difference in the CO values between esCCO and ICO was −0.39 ± 1.15 L min−1 (percentage error, 35.6 %). And corrected precision for repeated measures was 1.16 L min−1 (percentage error for repeated measures, 36.0 %). A concordance analysis showed that the concordance rate was 93.1 %. The mean angular bias was −1.8° and the radial limits of agreement were ±37.6°. The difference between the APCO and ICO CO values was 0.04 ± 1.37 L min−1 (percentage error, 42.4 %). And corrected precision for repeated measures was 1.37 L min−1 (percentage error for repeated measures, 42.5 %). The concordance rate was 89.7 %, with a mean angular bias of −3.3° and radial limits of agreement of ±42.2°. This study demonstrated that the trending ability of the esCCO system is not clinically acceptable, as judged by polar plots analysis; however, its trending ability is clinically acceptable based on a concordance analysis, and is comparable with currently available arterial waveform analysis methods.






Similar content being viewed by others
References
Foley R, Parfrey P, Sarnak M. Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol. 1998;9(12 Suppl):S16–23.
Pilmore H, Dent H, Chang S, McDonald S, Chadban S. Reduction in cardiovascular death after kidney transplantation. Transplantation. 2010;89:851–7.
U.S. Renal Data System, USRDS. 2009 annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2009.
Ducloux D, Kazory A, Chalopin JM. Predicting coronary heart disease in renal transplant recipients: a prospective study. Kidney Int. 2004;66:441–7.
Peyton PJ, Chong SW. Minimally invasive measurement of cardiac output during surgery and critical care: a meta-analysis of accuracy and precision. Anesthesiology. 2010;113:1220–35.
Funk DJ, Moretti EW, Gan TJ. Minimally invasive cardiac output monitoring in the perioperative setting. Anesth Analg. 2009;108:887–97.
Feldman JM. Is it a bird? Is it a plane? The role of patient monitors in medical decision making. Anesth Analg. 2008;108:707–10.
Ochiai R, Takeda J, Hosaka H, Sugo Y, Tanaka R, Soma T. The relationship between modified pulse wave transit time and cardiovascular changes in isoflurane anesthetized dogs. J Clin Monit Comput. 1999;15:493–501.
Sugo Y, Ukawa T, Takeda S, Ishihara H, Kazama T, Takeda Z. A novel continuous cardiac output monitor based on pulse wave transit time. Conf Proc IEEE Eng Med Biol Soc. 2010;2010:2853–6.
Critchley LA, Lee A, Ho AM. A critical review of the ability of continuous cardiac output monitors to measure trends in cardiac output. Anesth Analg. 2010;111:1180–92.
Yamada T, Tsutsui M, Sugo Y, Sato T, Akazawa T, Sato N, Yamashita K, Ishihara H, Takeda J. Multicenter study verifying a method of non-invasive continuous cardiac output measurement using pulse wave transit time: a comparison with intermittent bolus thermodilution cardiac output. Anesth Analg. 2012;115:82–7.
Bland JM, Altman DG. Agreement between methods of measurement with multiple observations per individual. J Biopharm Stat. 2007;17:571–82.
Critchley LA, Yang XX, Lee A. Assessment of trending ability of cardiac output monitors by polar plot methodology. J Cardiothorac Vasc Anesth. 2011;25:536–46.
Critchley LA, Critchley JA. A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J Clin Monit Comput. 1999;15:85–91.
Bataille B, Bertuit M, Mora M, Mazerolles M, Cocquet P, Masson B, Moussottai PE, Ginot J, Silva S, Larché J. Comparison of esCCO and transthoracic echocardiography for non-invasive measurement of cardiac output intensive care. Br J Anaesth. 2012;109:879–86.
Ishihara H, Okawa H, Tanabe K, Tsubo T, Sugo Y, Akiyama T, Takeda S. A new non-invasive continuous cardiac output trend solely utilizing routine cardiovascular monitors. J Clin Monit Comput. 2004;18:313–20.
Mansencal N, Delobelle J, Balagny P, Badie J, Ihaddaden M, Arslan M, Diboug O. Usefulness of a noninvasive cardiac output measurement using pulse wave transit time in coronary care unit. Int J Cardiol. 2013;168:4411–2.
Ishihara H, Tsutsui M. Impact of changes in systemic vascular resistance on a novel non-invasive continuous cardiac output measurement system based on pulse wave transit time: a report of two cases. J Clin Monit Comput. 2014;28:423–7.
Pearse R, Dawson D, Fawcett J, Rhodes A, Grounds RM, Bennet ED. Early goal-directed therapy after major surgery reduces complications and hospital stay. A randomised, controlled trial. Crit Care. 2005;9:R687–93.
Bundgaard-Nielsen M, Holte K, Secher NH, Kehlet H. Monitoring of perioperative fluid administration by individualized goal-directed therapy. Acta Anaesthesiol Scand. 2007;51:331–40.
Donati A, Loggi S, Preiser JC, Orsetti G, Münch C, Gabbanelli V, Pelaia P, Pietropaoli P. Goal-directed intraoperative therapy reduces morbidity and length of hospital stay in high-risk surgical patients. Chest. 2007;132:1817–24.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Informed consent and ethical approval
The present study was approved by the ethics committee of the Toho University Omori Medical Centre (Tokyo, Japan); written informed consent was obtained from the study participants. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Terada, T., Oiwa, A., Maemura, Y. et al. Comparison of the ability of two continuous cardiac output monitors to measure trends in cardiac output: estimated continuous cardiac output measured by modified pulse wave transit time and an arterial pulse contour-based cardiac output device. J Clin Monit Comput 30, 621–627 (2016). https://doi.org/10.1007/s10877-015-9772-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-015-9772-x