
Abstract
Background
Primary immunodeficiency diseases (PID) are a group of heterogeneous, rare, genetic, mainly childhood disorders that affect specific components of immune system leading to serious complications.
Objectives
This study is aimed at describing the prevalence and the categories of PID, the ages of onset and the diagnosis, the clinical presentations, the treatment modalities and the overall outcome of affected patients.
Materials and Methods
A retrospective study was conducted on 131 pediatric patients (aged 0–14 years) diagnosed with PID at Hamad General Hospital during a 15-year period (1998–2012).
Results
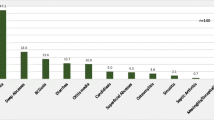
Data of 131 patients (75 males & 56 females) was analyzed with an estimated prevalence of 4.7 PID patients per 100,000 children younger than 14 years of age. The most common type of PID was predominantly antibody deficiency (23.7 %), followed by other well-defined immunodeficiency syndromes (22.9 %), 19.1 % combined T and B cell immunodeficiency, but rare CVID, and no cases of complement deficiency. The mean onset age was 24.01 months and diagnosis age was 42.2 months. Recurrent infections, particularly pneumonia (48.9 %), failure to thrive (34.4 %), otitis media (26 %), sepsis (23.7 %), and chronic diarrhoea (21.4 %) were commonest presenting conditions. P. aeruginosa (15.7 %), Salmonella species (13.2 %), and Non-TB mycobacteria (13.2 %) were the most common bacterial isolates. The overall mortality rate was 21.4 % with combined immunodeficiency’s accounting for 53.4 % of deaths.
Conclusions
This study reveals that PIDs are not rare in children in Qatar; and like other studies predominantly antibody deficiencies are the most common. Strategies that reinforce awareness and education of practicing physicians, bone marrow transplantation, and establishing PID national registry should be adopted to reduce mortality and morbidity of PID patients in Qatar.


Similar content being viewed by others


References
Rezaei N, Bonilla FA, Sullivan KE, et al. Chapter 1. An introduction to primary immunodeficiency diseases. In: Nima R, Asghar A, Notarangelo LD, editors. Primary immunodeficiency diseases, definition diagnosis and management. Berlin: Springer; 2008. p. 1–38.
Rezaei N, Hedayat M, Aghamohammadi A, Nichols KE. Primary immunodeficiency diseases associated with increased susceptibility to viral infections and malignancies. J Allergy Clin Immunol. 2011;127:1329–41.e2; quiz 1342–3.
Leechawengwongs E, Shearer WT. Lymphoma complicating primary immunodeficiency syndromes. Curr Opin Hematol. 2012;19:305–12.
Goyal R, Bulua A, Nikolov N, et al. Rheumatologic and autoimmune manifestations of primary immunodeficiency disorders. Curr Opin Rheumatol. 2009;21:78–84.
Joshi AY VV, Hagan JB, St Sauver JL, Boyce TG. Incidence and temporal trends of primary immunodeficiency: a population-based cohort study. Mayo Clin Proc. 2009;84:16–22.
Nourijelyani K, Aghamohammadi A, Sadaghiani MS, et al. Physicians awareness on primary immunodeficiency disorders in Iran. Iran J Allergy Asthma Immunol. 2012;11:57–64.
de Vries E, European Society for Immunodeficiencies (ESID) members. Patient-centred screening for primary immunodeficiency, a multi-stage diagnostic protocol designed for non-immunologists: 2011 update. Clin Exp Immunol. 2012;167:108–19.
Modell V, Gee B, Lewis DB et al. Global study of primary immunodeficiency diseases (PI)-diagnosis, treatment, and economic impact: an updated report from the Jeffrey Modell Foundation. Immunol Res 2011; 61–70.
Yüksek M, Ikincioğullari A, Doğu F, et al. Primary immune deficiency disease awareness among a group of Turkish physicians. Turk J Pediatr. 2010;52:372–7.
Reda SM, Afifi HM, Amine MM. Primary immunodeficiency diseases in Egyptian children: a single-center study. J Clin Immunol. 2008;29:343–51.
Barbouche MR, Galal N, Ben-Mustapha I, et al. Primary immunodeficiencies in highly consanguineous North African populations. Ann N Y Acad Sci. 2011;1238:42–52.
Aghamohammadi A, Moin M, Rezaei N. History of primary immunodeficiency diseases in Iran. Iran J Pediatr. 2010;20:16–34.
Rezaei N, Aghamohammadi A, Moin M, et al. Frequency and clinical manifestations of patients with primary immunodeficiency disorders in Iran: update from the Iranian Primary Immunodeficiency Registry. J Clin Immunol. 2006;26:519–32.
Dar-Odeh NS, Hayajneh WA, Abu-Hammad OA, et al. Orofacial findings in chronic granulomatous disease: report of twelve patients and review of the literature. BMC Res Notes. 2010;17:37.
Al-Herz W. Primary immunodeficiency disorders in Kuwait: first report from Kuwait National Primary Immunodeficiency Registry (2004–2006). J Clin Immunol. 2008;28:186–93.
Al-Herz W, Zainal M, Salama M, et al. Primary immunodeficiency disorders: survey of pediatricians in Kuwait. J Clin Immunol. 2008;28:379–83.
Al-Herz W, Bousfiha A, Casanova JL, et al. Primary immunodeficiency diseases: an update on the classification from the international union of immunological societies expert committee for primary immunodeficiency. Front Immunol. 2011;2:54. Epub 2011 Nov 2018.
http://www.esid.org/clinical-diagnostic-criteria-for-pid-73-0.
Ehlayel M, de Beaucoudrey L, Fike F, et al. Simultaneous presentation of 2 rare hereditary immunodeficiencies: IL-12 receptor beta1 deficiency and ataxia-telangiectasia. J Allergy Clin Immunol. 2008;122:1217–9.
Meller J, Malinin NL, Panigrahi S, et al. Novel aspects of Kindlin-3 function in humans based on a new case of leukocyte adhesion deficiency III (LAD-III). J Thromb Haemost. 2012;10:1397–408.
Statistical Authority of Qatar. www.qsa.gov.qa [Last visited July 5th, 2012].
Qatar Financial Centre Authority. www.qfc.com.qa [Last visited July 5th, 2012].
Naidoo R, Ungerer L, Cooper M, et al. Primary immunodeficiencies: a 27-year review at a tertiary paediatric hospital in Cape Town, South Africa. J Clin Immunol. 2011;31:99–105.
Gupta S, Madkaikar M, Singh S, Sehgal S. Primary immunodeficiencies in India: a perspective. Ann N Y Acad Sci. 2012;1250:73–9.
Leiva LE, Zelazco M, Oleastro M, et al. Primary immunodeficiency diseases in Latin America: the second report of the LAGID registry. J Clin Immunol. 2007;27:101–8.
Golan H, Dalal I, Garty BZ, et. al. The incidence of primary immunodeficiency syndromes in Israel. Isr Med Assoc J 2002; 868–871.
Sanal O, Tezcan I. Thirty years of primary immunodeficiencies in Turkey. Ann N Y Acad Sci. 2011;1238:15–23.
Al-Tamemi S, Ibtisam E, Dennison D. Primary immunodeficiency diseases in Oman: five years’ experience at Sultan Qaboos University Hospital. World Allergy Organ J. 2012;5:52–6.
Al-Muhsen S, Casanova JL. The genetic heterogeneity of mendelian susceptibility to mycobacterial diseases. J Allergy Clin Immunol. 2008;122:1043–51.
Fieschi C, Dupuis S, Catherinot E, et al. Low penetrance, broad resistance, and favorable outcome of interleukin 12 receptor beta1 deficiency: medical and immunological implications. J Exp Med. 2003;197:527–35.
Lee WI, Kuo ML, Huang JL, et al. Distribution and clinical aspects of primary immunodeficiencies in a Taiwan pediatric tertiary hospital during a 20-year period. J Clin Immunol. 2005;25:162–73.
Acknowledgments
The authors would like to thank Hamad Medical Corporation for their support and ethical approval (HMC Research Protocol No. 10078/10)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ehlayel, M.S., Bener, A. & Laban, M.A. Primary Immunodeficiency Diseases in Children: 15 Year Experience in a Tertiary Care Medical Center in Qatar. J Clin Immunol 33, 317–324 (2013). https://doi.org/10.1007/s10875-012-9812-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-012-9812-y