
Abstract
Purpose
Left atrial volume (LA) and pulmonary vein (PV) anatomy may potentially relate to technical challenges in achieving stable and effective catheter position in case of atrial fibrillation (AF) ablation by means of “one-shot” catheters. The aim of this study was to investigate whether LA volume and PV anatomy, evaluated by computed tomography (CT) or magnetic resonance (MR) prior to ablation, predict acute and midterm outcome of AF ablation by nMARQ™.
Methods
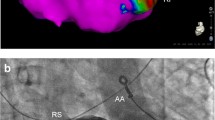
We included 75 patients (mean age 58 ± 11 years, 67 % male) with symptomatic paroxysmal AF. All patients underwent CT/MR scanning prior to catheter ablation to evaluate LA volume and PV anatomy. All the patients underwent PV isolation by nMARQ™, an open-irrigated mapping and radiofrequency (RF) decapolar ablation catheter. Ablation was guided by electroanatomic mapping allowing RF energy delivery in the antral region of PVs from ten irrigated electrodes simultaneously.
Results
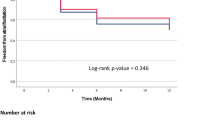
Mean LA volume was 75 ± 40 ml. A normal anatomy (4 PVs) was documented in 40 (53 %) patients and abnormal anatomy (common truncus or accessory PVs) in 35 patients. Mean procedural and fluoroscopy times were 94 ± 55 and 8 ± 5 min, respectively, without significant differences among patients with normal or abnormal anatomy (92 ± 45 vs 95 ± 64 min, p = 0.85 and 6 ± 3 vs 8 ± 4 min, p = 0.65, respectively). Mean ablation time was 14 ± 3 min, and 99 % of the targeted veins were isolated with a mean of 23 ± 5 RF pulses per patient. After a mean follow-up of 17 ± 8 months, 23 (31 %) patients had an atrial arrhythmia recurrence. Neither LA volume nor PV anatomy was a predictor of outcome.
Conclusions
LA volume and PV anatomy did not affect procedural data and outcome in patients who underwent PV isolation by an open-irrigated mapping and RF decapolar ablation catheter.





Similar content being viewed by others

References
Camm AJ, Lip GYH, De Caterina R, Savelieva I, Atar D, Honloser SH, et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation. An update of the 2010 ESC guidelines for the management of atrial fibrillation. Europace. 2012;14:1385–413.
January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland Jr JC, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–104.
Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al. Heart Rhythm Society Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. 2012 HRS/EHRA/ECAS Expert Consensus Statement 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Heart Rhythm. 2012;9:632–96.
Sarabanda AV, Bunch TJ, Johnson SB, Mahapatra S, Milton MA, Leite LR, et al. Efficacy and safety of circumferential pulmonary vein isolation using a novel cryothermal balloon ablation system. J Am Coll Cardiol. 2005;46:1902–12.
De Filippo P, He DS, Brambilla R, Gavazzi A, Cantù F. Clinical experience with a single catheter for mapping and ablation of pulmonary vein ostium. J Cardiovasc Electrophysiol. 2009;20:367–73.
Dukkipati SR, Kuck KH, Neuzil P, Woollett I, Kautzner J, McElderry HT, et al. Pulmonary vein isolation using a visually guided laser balloon catheter: the first 200-patient multicenter clinical experience. Circ Arrhythm Electrophysiol. 2013;6:467–72.
Deneke T, Schade A, Müller P, Schmitt R, Christopoulos G, Krug J, et al. Acute safety and efficacy of a novel multipolar irrigated radiofrequency ablation catheter for pulmonary vein isolation. J Cardiovasc Electrophysiol. 2014;25:339–45.
Anselmino M, Blandino A, Beninati S, Rovera C, Boffano C, Belletti M, et al. Morphologic analysis of left atrial anatomy by magnetic resonance angiography in patients with atrial fibrillation: a large single center experience. J Cardiovasc Electrophysiol. 2011;22:1–7.
den Uijl DW, Tops LF, Delgado V, Schuijf JD, Kroft LJ, de Roos A, et al. Effect of pulmonary vein anatomy and left atrial dimensions on outcome of circumferential radiofrequency catheter ablation for atrial fibrillation. Am J Cardiol. 2011;107:243–9.
Stabile G, De Ruvo E, Grimaldi M, Rovaris G, Soldati E, Anselmino M, et al. Safety and efficacy of pulmonary vein isolation using a circular, open-irrigated mapping and ablation catheter: a multicenter registry. Heart Rhythm. 2015;12:1782–8.
Bertaglia E, Stabile G, Senatore G, Zoppo F, Turco P, Amellone C, et al. Predictive value of early atrial fibrillation recurrence after circumferential pulmonary vein ablation. Pacing Clin Electrophysiol. 2005;28:366–71.
Kato R, Lickfett L, Meininger G, Dickfeld T, Wu R, Juang G, et al. Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: lessons learned by use of magnetic resonance imaging. Circulation. 2003;107:2004–10.
Micochova H, Tintera J, Porod V, Peichl P, Cihak R, Kautzner J. Magnetic resonance angiography of pulmonary veins: Implications for catheter ablation of atrial fibrillation. Pacing Clin Electrophysiol. 2005;28:1073–80.
Marom EM, Herndon JE, Kim YH, McAdams HP. Variations in pulmonary venous drainage to the left atrium: implications for radiofrequency ablation. Radiology. 2004;230:824–9.
Mansour M, Refaat M, Heist EK, Mela T, Cury R, Holmvang G, et al. Three-dimensional anatomy of the left atrium by magnetic resonance angiography: implication for catheter ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2006;17:719–23.
Wazni OM, Tsao HM, Chen SA, Chaung HH, Saliba W, Natale A, et al. Cardiovascular imaging in the management of atrial fibrillation. J Am Coll Cardiol. 2006;48:2077–84.
Anselmino M, Scaglione M, Blandino A, Beninati S, Caponi D, Boffano C, et al. Pulmonary veins branching pattern, assessed by magnetic resonance, does not affect transcatheter atrial fibrillation ablation outcome. Acta Cardiol. 2010;65:665–74.
McLellan AJ, Ling LH, Ruggiero D, Wong MC, Walters TE, Nisbet A, et al. Pulmonary vein isolation: the impact of pulmonary venous anatomy on long-term outcome of catheter ablation for paroxysmal atrial fibrillation. Heart Rhythm. 2014;11:549–56.
Tsyganov A, Petru J, Skoda J, Sediva L, Hala P, Weichet J, et al. Anatomical predictors for successful pulmonary vein isolation using balloon-based technologies in atrial fibrillation. J Interv Card Electrophysiol. 2015;4:265–71.
Metzner A, Kivelitz D, Schmidt B, Fuernkranz A, Wissner E, Tilz RR, et al. Impact of pulmonary vein anatomy assessed by cardiac magnetic resonance imaging on endoscopic pulmonary vein isolation in consecutive patients. Europace. 2012;14:474–80.
Schmidt M, Dorwarth U, Straube F, Daccarett M, Rieber J, Wankerl M, et al. Cryoballoon in AF ablation: impact of PV ovality on AF recurrence. Int J Cardiol. 2013;167:114–20.
Kubala M, Hermida JS, Nadji G, Quenum S, Traulle S, Jarry G. Normal pulmonary vein anatomy is associated with better AF free survival after cryoablation as compared to atypical anatomy with common left pulmonary vein. Pacing Clin Electrophysiol. 2011;34:837–43.
Sorgente A, Chierchia GB, de Asmundis C, Sarkozy A, Namdar M, Capulzini L, et al. Pulmonary vein ostium shape and orientation as possible predictors of occlusion in patients with drug-refractory paroxysmal atrial fibrillation undergoing cryoballoon ablation. Europace. 2011;13:205–12.
Merchant FM, Levy MR, Iravanian S, Clermont EC, Kelli HM, Eisner RL, et al. Pulmonary vein anatomy assessed by cardiac magnetic resonance imaging in patients undergoing initial atrial fibrillation ablation: implications for novel ablation technologies. J Interv Card Electrophysiol. 2016 Jan 26. [Epub ahead of print]
Faletti R, Rapellino A, Barisone F, Anselmino M, Ferraris F, Fonio P, et al. Use of oral gadobenate dimeglumine to visualise the oesophagus during magnetic resonance angiography in patients with atrial fibrillation prior to catheter ablation. J Cardiovasc Magn Reson. 2014;16:41.
Hof I, Arbab-Zadeh A, Scherr D, Chilukuri K, Dalal D, Abraham T, et al. Correlation of left atrial diameter by echocardiography and left atrial volume by computed tomography. J Cardiovasc Electrophysiol. 2009;20:159–63.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by the institutional review committees, and all patients signed informed consents. The principle outlined in latest update of the Declaration of Helsinki was followed.
Conflict of interest
The authors declare that they have no conflict of interest.
Appendix
Appendix
Participating centers:
Clinica Mediterranea, Napoli (Giuseppe Stabile, Assunta Iuliano, Alfonso Panella); Policlinico Casilino, Roma (Leonardo Calò, Gildo De Ruvo, Luigi Sciarra); Azienda Ospedaliero Universitaria Pisana, Pisa (Ezio Soldati, Maria Grazia Bongiorni); Dipartimento di Scienze Mediche, Università di Torino (Matteo Anselmino, Federico Ferraris, Fiorenzo Gaita); Clinica Montevergine, Mercogliano (AV) (Francesco Solimene).
Rights and permissions
About this article

Cite this article
Stabile, G., Anselmino, M., Soldati, E. et al. Effect of left atrial volume and pulmonary vein anatomy on outcome of nMARQ™ catheter ablation of paroxysmal atrial fibrillation. J Interv Card Electrophysiol 48, 201–207 (2017). https://doi.org/10.1007/s10840-016-0189-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-016-0189-3