
Abstract
Background
There is scant data about outcomes in patients with left ventricular epicardial (LVE) leads who develop endocarditis or device-related infection.
Objective
This retrospective study evaluated mortality and recurrence of infection among patients with LVE leads in comparison to patients with endovascular coronary sinus (CS) leads after the development of endocarditis or device-related infection.
Methods
Patients with cardiac resynchronization therapy (CRT) devices who developed endocarditis or pocket infection over 5 years at Cleveland Clinic were included in the study. The groups were all patients with LVE leads versus CRT devices without epicardial leads that developed endocarditis or pocket infection. Mortality was assessed using the Social Security Death Index and re-infection was assessed by reviews of the medical record.
Results
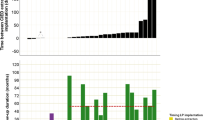
Prospective extraction of the CRT device and leads occurred among all 50 patients with CS leads and 8 of the 14 patients with LVE leads. The survival rate was 92.9 versus 92 % and freedom from re-infection rate was 64.3 versus 80 % in the patients with LVE leads versus CS leads, respectively, over 1 year (P value = 0.918 and 0.226, respectively). At 3 years, the survival rate in LVE lead group was 92.9 % and freedom from re-infection rate was 64.3 % in comparison to survival rate of 90 % and freedom from re-infection rate of 68 % in the CS group (P value = 0.751 and 0.798, respectively).
Conclusion
After development of endocarditis or pocket infection, no statistically significant differences were seen in mortality, or recurrent infection between patients with LVE leads and those with CS leads.


Similar content being viewed by others
References
Nery, P. B., Fernandes, R., Nair, G. M., Sumner, G. L., Ribas, C. S., Menon, S. M., et al. (2010). Device-related infection among patients with pacemakers and implantable defibrillators: incidence, risk factors, and consequences. Journal of Cardiovascular Electrophysiology, 21, 786–790.
Baddour, L. M., Epstein, A. E., Erickson, C. C., Knight, B. P., Levison, M. E., Lockhart, P. B., et al. (2011). A summary of the update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association. Journal of the American Dental Association, 142, 159–165.
Fernandez, A. L., Garcia-Bengochea, J. B., Ledo, R., Vega, M., Amaro, A., Alvarez, J., et al. (2004). Minimally invasive surgical implantation of left ventricular epicardial leads for ventricular resynchronization using video-assisted thoracoscopy. Revista Española de Cardiología, 57, 313–319.
Mair, H., Jansens, J. L., Lattouf, O. M., Reichart, B., & Dabritz, S. (2003). Epicardial lead implantation techniques for biventricular pacing via left lateral mini-thoracotomy, video-assisted thoracoscopy, and robotic approach. The Heart Surgery Forum, 6, 412–417.
Mair, H., Kaczmarek, I., Oberhoffer, M., & Daebritz, S. (2006). Minimally invasive surgical placement of left ventricular epicardial lead: letter 2. Annals of Thoracic Surgery, 81, 407–408.
Matsumoto, Y., Akemoto, K., Ushijima, T., Kawakami, K., Ueyama, T., & Sasaki, H. (1998). Removal of infected pacemaker lead through sternotomy without cardiopulmonary bypass. The Japanese Journal of Thoracic and Cardiovascular Surgery, 46, 71–74.
Daoud, E. G., Strickberger, S. A., Man, K. C., Bolling, S. F., Kirsh, M. M., Morady, F., et al. (1995). Comparison of early and late complications in patients undergoing coronary artery bypass graft surgery with and without concomitant placement of an implantable cardioverter defibrillator. American Heart Journal, 130, 780–785.
Zipes, D. P., & Roberts, D. (1995). Results of the international study of the implantable pacemaker cardioverter-defibrillator. A comparison of epicardial and endocardial lead systems. The pacemaker-cardioverter-defibrillator investigators. Circulation, 92, 59–65.
Byrd, C. L. (2001). Advances in device lead extraction. Current Cardiology Reports, 3, 324.
Klug, D., Lacroix, D., Savoye, C., Goullard, L., Grandmougin, D., Hennequin, J. L., et al. (1997). Systemic infection related to endocarditis on pacemaker leads: clinical presentation and management. Circulation, 95, 2098–2107.
Voet, J. G., Vandekerckhove, Y. R., Muyldermans, L. L., Missault, L. H., & Matthys, L. J. (1999). Pacemaker lead infection: report of three cases and review of the literature. Heart, 81, 88–91.
Choo, M. H., Holmes, D. R., Jr., Gersh, B. J., Maloney, J. D., Merideth, J., Pluth, J. R., et al. (1981). Infected epicardial pacemaker systems. Partial versus total removal. Journal of Thoracic and Cardiovascular Surgery, 82, 794–796.
Shimizu, H., Yozu, R., Ueda, T., Goto, T., Soma, Y., & Kawada, S. (1994). Removal of infected total pacemaker system under extracorporeal circulation–a case report and review of the Japanese literature. Nihon Kyobu Geka Gakkai Zasshi, 42, 160–165.
Suzuki, T., Kawai, H., Takabayashi, A., Miyake, Y., Maze, Y., Kondoh, T., et al. (2001). Total removal of infected pacemaker lead under cardiopulmonary bypass in a case of endocarditis, bacteremia and lung abscess. Kyobu Geka, 54, 428–431.
Conflict of interest
Bruce L. Wilkoff, MD, is an unpaid consultant for Spectranetics Inc, Medtronic Inc., and St. Jude Medical.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karim, S., Hussein, A., Batal, O. et al. Outcomes after endocarditis or device infection in patients with left ventricular epicardial leads versus coronary sinus leads. J Interv Card Electrophysiol 39, 267–271 (2014). https://doi.org/10.1007/s10840-014-9880-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-014-9880-4