
Abstract
Purpose
Current re-introduction of “improved” preimplantation genetic screening (PGS#2) raises the question whether PGS#2 is ready for routine clinical application.
Methods
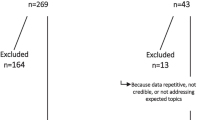
We assessed available evidence via review of published data for years 2005–2012, and review of currently ongoing registered clinical trials, based on searches under appropriate key words in PubMed, MEDLINE, Cochrane Database System Review and Google Scholar and http://www.ClinicalTrials.gov. In absence of prospective clinical trials, and due to limited available data, individual publications/ongoing studies are assessed.
Results
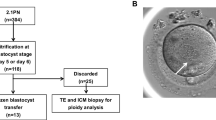
PGS#2 offers significant improvements in accuracy of aneuploidy diagnosis over PGS#1. By moving embryo biopsy from day-3 after fertilization (6–8 cell stage) to trophectoderm biopsy at blastocyst stage (day 5–6), PGS#2, however, adds additional co-variables to the analysis of efficacy of the procedure, which have special relevance for women with diminished ovarian reserve (DOR), who usually produce small egg and embryo numbers. Limited published data, claiming efficacy of PGS#2, as well as ongoing clinical trials, do not consider these additional co-variables, do not analyze outcomes by intent to treat and, therefore, have to be considered biased in patient selection.
Conclusions
Here reached conclusions are based on absence of adequate data rather than affirmative outcome assessments. They, therefore, are subject to change at any future date with generation of significant new data. Premature introduction of PGS#1 caused significant damage to patients. As currently no reliable PGS#2 data are available to suggest improvements in IVF outcomes, to avoid a repeat of the PGS#1 experience, PGS#2 should be considered experimental until data show otherwise.
Similar content being viewed by others

References
Gleicher N, Weghofer A, Barad D. Preimplantation genetic screening: “established” and ready fro prime time? Fertil Steril. 2008;89:780–8.
Mastenbroek S, Twisk M, van Echten-Arends J, Sikkema-Raddatz B, Korevaar JC, Verhoeve HR, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med. 2007;357:9–17.
Hardarson T, Hanson C, Lundin K, Hillensjö T, Nilsson L, Stevic J, et al. Preimplantation genetic screening in women of advanced maternal age caused a decrease in clinical pregnancy rate: a randomized controlled trial. Hum Reprod. 2008;23:2806–12.
Mayer LR, Klipstein S, Hazlett WD, Nasta T, Mangan P, Karande V. A prospective randomized controlled trial of preimplantation genetic screening in the “good prognosis” patient. Fertil Steril. 2009;91:1731–8.
Debrock S, Melotte C, Spiessens C, Peeraer K, Vanneste E, Meeuwis L, et al. Preimplantation genetic screening for aneuploidy of embryos after in vitro fertilization in women aged at least 35 years: a prospective randomized trial. Fertil Steril. 2010;93:364–73.
Mastenbroek S, Twisk M, van der Veen F, Repping S. Preimplantation genetic screening: a systematic review and meta-analysis of RCTs. Huma Reprod Update. 2011;17:454–4566.
Anderson RA, Pickering S. The current status of preimplantation genetic screening: British Fertility Society Policy and Practice Guidelines. Hum Fertil (Camb). 2008;11:71–5.
Practice Committee of Society for Assisted Reproductive Technology, Practice Committee of American Society for Reproductive Medicine. Preimplantation genetic testing: a practice committee opinion. Fertil Steril. 2008;90(5 Suppl):S136–43.
Harper J, Coonen E, de Rycke M, Fiorentino F, Geraedts J, Goossens V, et al. What next for preimplantation genetic screening (PGS)? A position statement from the ESHRE PGD Consortium Steering Commmitttee. Hum Reprod. 2010;25:821–3.
Gleicher N, Kim A, Weghofer A, Barad DH. Lessons from elective in vitro fertilization (IVF) in, principally, non-infertile women. Reprod Biol Endocrinol. In press
Fragouli E, Katz-Jaffe M, Alfarawati S, Stevens J, Colls P, Goodall NN et al. Comprehensive chromosome screening of polar bodies and blastocysts from couples experiencing repeated implantation failure. Fertil Steril. ;94:875–87.
Schoolcraft WB, Fragouli E, Stevens J, Munné S, Katz-Jaffe MG, Wells D. Clinical application of comprehensive chromosomal screening at the blastocyst stage. Fertil Steril. 2010;94:1700–6.
Rius M, Daina G, Obradors A, Ramos L, Velilla E, Fernández S, et al. Comprehensive embryo analysis of advanced maternal age-related aneuploidies and mosaicism by short genomic hybridization. Fertil Steril. 2011;95:413–6.
Brezina PR, Benner A, Rechitsky S, Kuliev A, Pomerantseva E, Pauling D, et al. Single-gene testing combined with single nucleotide polymorphism microarray preimplantation genetic diagnosis for enuploidy: a novel approach in optimizing pregnancy outcome. Fertil Steril. 2011;95:1786e5–8.
Scott Jr RT, Ferry K, Su J, Tao X, Scott K, Treff NR. Comprehensive chromosome screening is highly predictive of the reproductive potential of human embryos: a prospective, blinded, nonselection study. Fertil Steril. 2012;97:870–5.
Yang Z, Liu J, Collins GS, Salem SA, Liu X, Lyle SS, et al. Selection of sinle blastocysts for fresh transfer via standard morphology assessment alone and with array CGH for good prognosis IVF patients: results from a randomized pilot study. Mol Cytogenet. 2012;5:24.
Milán M, Cobo AC, Rodrigo L, Mateu E, Mercader A, Buendia P, et al. Redefining advanced maternal age as an indication for preimplantation geneic screening. Reprod Biomed Online. 2010;21:649–57.
Rabinowitz M, Ryan A, Gemelos G, Hill M, Baner J, Cinnioglu C, et al. Origins and rates of aneuploidy in human blastomeres. Fertil Steril. 2012;97:395–401.
Treff NR, Tao X, Ferry KM, Su J, Taylor D, Scott Jr RT. Development and validation of an accurate quantitative real-time polymerase chain reaction-based assay for human blastocyst comprehensive chromosomal aneuploidy screening. Fertil Steril. 2019;97:819–24.
Verlinsky Y, Kuliev A. Preimplantation diagnosis for aneuploidies in assisted reproduction. Minerva Ginecol. 2004;56:197–203.
Kuliev A, Cieslak J, Verlinsky Y. Frequency and distribution of chromosome abnormalities in human oocytes. Cytogenet Genome Res. 2005;111:193–8.
Verlinsky Y, Cieslak J, Freidine M, Ivakhnenko V, Wolf G, Kovalinskaya L, et al. Polar body diagnosis of common aneuploidies by FISH. J Assist Reprod Genet. 1996;13:57–162.
Verlinsky Y, Cieslak J, Ivakhnenko V, Evsikov S, Wolf G, White M, et al. Prepregnancy genetic testing for age-related aneuploidies by polar body analysis. Genet Test. 1997–1998;1:231–5.
Cohen J, Wells D, Munné S. Removal of 2 cells from cleavage stage embryos is likely to reduce the efficacy of chromosomal tests that are used to enhance implantation rates. Fertil Steril. 2007;87:496–503.
Baart EB, Martini E, van den Berg I, Macklon NS, Galijaard RJ, Fauser BC, et al. Preimplantation genetic screening reveals a high incidence of aneuploidy and mosaicism in embryos from young women undergoing IVF. Hum Reprod. 2006;21:223–33.
Munné S, Fragouli E, Colls P, Katz-Jaffe M, Schoolcraft W, Wells D. Improved detection of aneuploid blastocysts using a new 12-chromosome FISH test. Reprod Biomed Online. 2010;20:92–7.
McArthur SJ, Leigh D, Marshall JT, de Boer KA, Jansen RP. Oregnancies and live births after trophectoderm biopsy and preimplantation genetic testing of human blastocysts.
Gutiérrez-Mateo C, Wells D, Benet J, Sánchez-García JF, Bermúdez MG, Belil I, et al. Reliability of comparative genomic hybridization to detect chromosome abnormalities in first polar bodies and metaphase II oocytes. Hum Reprod. 2004;19:2118–25.
Geraedts J, Collins J, Gianaroli L, Goossens V, Handyside A, Harper J, et al. What next for preimplantation genetic screening? A polar body approach? Hum Reprod. 2010;25:575–7.
Harper JC, Harton G. The use of arrays in preimplantation genetic diagnosis and screening. Fertil Steril. 2010;94:1173–7.
Schoolcraft WB, Treff NR, Stevens JM, Ferry K, Katz-Jaffe M, Scott Jr RT. Live birth outcome with trophectoderm biopsy, blastocyst vitrification, and single-nucleotide polymorphism microarray-based comprehensive chromosome screening in infertile patients. Fertil Steril. 2011;96:638–40.
Schoolcraft WB, Katz-jaffe MG, Stevens J, Rawlins M, Munné S. Preimplantation aneuploidy testing for infertile patients of advanced maternal age; a randomized prospective trial. Fertil Steril. 2009;92:157–62.
Twisk M, Mastenbroek S, van Wely M, Heineman MJ, Van der Veen F, Repping S. Preimplantation genetic screening for abnormal number of chromosomes (aneuploidies) in in vitro fertilization or intracytoplasmic sperm injection. Cochrane Database Syst Rev. 2006;(1):CD005291
Musters AM, Repping S, Korevaar JC, Mastenbroek S, Limpens J, van der Veen F, et al. Pregnancy outcome after preimplantation genetic screening or natural conception in couples with unexplained recurrent miscarriages: a systematic review of the best available evidence. Fertil Steril. 2011;95:2153–7.
Ly KD, Agarwal A, Nagy ZP. Preimplantation genetic screening: does it help or hinder IVF treatment and what is the role of the embryo? J Assist Reprod Genet. 2011;28:833–49.
Harper JC, Sengupta SB. Preimplantation genetic diagnosis: state of the art 2011. Hum Genet. 2012;131:175–86.
Blake DA, Farquhar CM, Johnson N, Proctor M. Cleavage stage versus blastocyst stage embryo transfer in assisted conception. Cochrane Database Syst Rev. 2007;CD002118
Barad DH, Weghofer A, Gleicher N. Age-specific levels for basal follicle-stimulating hormone assessment of ovarian function. Obstet Gynecol. 2007;109:1404–10.
Barad DH, Weghofer A, Gleicher N. Utility of age-specific serum anti-Müllerian hormone concentrations. Reprod Biomed Online. 2011;22:284–91.
Funding
This study was supported by extramural funds from the Foundation for Reproductive Medicine and intramural funds from the Center for Human Reproduction (CHR) New York.
Conflict statement
The authors have no conflict to declare in regards to here published materials.
Author information
Authors and Affiliations
Corresponding author
Additional information
Norbert Gleicher and David H. Barad contributed equally to the work.
Capsule
Though the current re-introduction of preimplantation genetic screening (PGS) involves greatly improved aneuploidy testing of embryos, currently available data do not demonstrate outcome improvements for in vitro fertilization (IVF). Until such data become available, PGS, therefore, should be considered an experimental procedure.
Rights and permissions
About this article
Cite this article
Gleicher, N., Barad, D.H. A review of, and commentary on, the ongoing second clinical introduction of preimplantation genetic screening (PGS) to routine IVF practice. J Assist Reprod Genet 29, 1159–1166 (2012). https://doi.org/10.1007/s10815-012-9871-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-012-9871-2