
Abstract
Background
Placement of covered self-expandable metallic stent (CSEMS) for post-endoscopic sphincterotomy (ES) bleeding achieves excellent hemostasis results. Although CSEMS placement is typically performed after failure of conventional endoscopic combination therapy, its excellent outcomes may justify earlier placement.
Aims
We aimed to examine the efficacy of “early” CSEMS placement for massive post-ES bleeding.
Methods
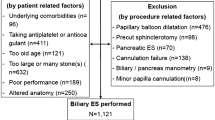
The medical records of 2750 patients who underwent ES between 2005 and 2019 were reviewed retrospectively, and 61 patients who developed massive post-ES bleeding were enrolled. These patients were divided into those who underwent early CSEMS placement (E-CSEMS group) and those who underwent conventional endoscopic combination therapy (Conventional group). The outcomes of hemostasis procedures were compared between the groups.
Results
The primary success rates of endoscopic hemostasis were 100% (21/21) and 98% (39/40) in the E-CSEMS group and Conventional group, respectively, without significant differences (P = 1.000). However, in the E-CSEMS group, re-bleeding was significantly less frequent (5% vs. 31%; P = 0.023), the median hemostasis procedure time was significantly shorter (14 min vs. 26 min; P < 0.001), and transfusion after initial hemostasis treatment was less commonly required (10% vs. 38%; P = 0.034). Multivariate analyses showed that hemodialysis was associated with a significantly higher re-bleeding rate (P = 0.029), while CSEMS placement was associated with a significantly lower re-bleeding rate (P = 0.039).
Conclusions
Early CSEMS placement may be effective for improving the clinical outcomes of massive post-ES bleeding by decreasing re-bleeding and the extent of bleeding.



Similar content being viewed by others


References
Freeman ML, Melson DB, Sherman S, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–918.
Loperfido S, Angelini G, Benedetti G, et al. Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastrointest Endosc. 1998;48:1–10.
Masci EN, Toti G, Mariani A, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001;96:417–423.
Chandrasekhara V, Khashab MA, Muthusamy VR, et al. Adverse events associated with ERCP. Gastrointest Endsoc. 2017;85:32–47.
Ferreira LE, Baron TH. Post-sphincterotomy bleeding: who, what, when, and how. Am J Gastroenterol. 2007;102:2850–2858.
Lee MH, Tsou YK, Lin CH, et al. Predictors of re-bleeding after endoscopic hemostasis for delayed post-endoscopic sphincterotomy bleeding. World J Gastroenterol. 2016;22:3196–3201.
Maleux G, Bielen J, Laenen A, et al. Embolization of post-biliary sphincterotomy bleeding refractory to medical and endoscopic therapy: technical results, clinical efficacy and predictors of outcome. Eur Radiol. 2014;24:2779–2786.
Shah JN, Marson F, Binmoeller KF. Temporary self-expandable metal stent placement for treatment of post-sphincterotomy bleeding. Gastrointest Endosc. 2010;72:1274–1278.
Itoi T, Yasuda I, Doi S, et al. Endoscopic hemostasis using covered metallic stent placement for uncontrolled post-endoscopic sphincterotomy bleeding. Endoscopy. 2011;43:369–372.
Canena J, Liberato M, Horta D, et al. Short-term stenting using fully covered self-expandable metal stents for treatment of refractory biliary leaks, postsphincterotomy bleeding, and perforations. Surg Endosc. 2013;27:313–324.
Cochrane J, Schlepp G. Comparing endoscopic intervention against fully covered self-expanding metal stent placement for post-endoscopic sphincterotomy bleed (CEASE Study). Endosc Int Open. 2016;4:E1261–E1264.
Huang PT, Tsai MH, Chen TM, et al. Management of postendoscopic sphincterotomy bleeding with fully covered self-expanding metal stent. Adv Dig Med. 2019;6:53–57.
Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–454.
Iwasaki E, Itoi T, Kanai T. Metal stent for refractory post-ES bleeding: is this the ultimate treatment modality? Endosc Int Open. 2016;4:E1265–E1266.
Kim KO, Kim TN, Kim SB, et al. Characteristics of delayed hemorrhage after endoscopic sphincterotomy. J Gastroenterol Hepatol. 2010;25:532–538.
Hori Y, Naitoh I, Nakazawa T, et al. Feasibility of endoscopic retrograde cholangiopancreatography-related procedure in hemodialysis patients. J Gastroenterol Hepatol. 2014;29:648–652.
Ikarashi S, Katanuma A, Kin T, et al. Factors associated with delayed hemorrhage after endoscopic sphincterotomy: Japanese large single-center experience. J Gastroenterol. 2017;52:1258–1265.
Muro S, Kato H, Ishida E, et al. Comparison of anticoagulants and risk factors for bleeding following endoscopic sphincterotomy among anticoagulant users: results from a large multicenter retrospective study. J Gastroenterol Hepatol. 2019. https://doi.org/10.1111/jgh.14764.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Inoue, T., Ibusuki, M., Kitano, R. et al. Early Covered Self-Expandable Metal Stent Placement Is Effective for Massive Post-endoscopic Sphincterotomy Bleeding. Dig Dis Sci 65, 3324–3331 (2020). https://doi.org/10.1007/s10620-020-06057-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06057-0