
Abstract
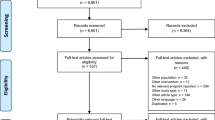
Overall survival (OS) has been debated as the most important clinical endpoint in metastatic breast cancer (MBC) trials mainly because survival could be influenced by treatment after progression in an era of effective subsequent-line agents. We conducted a search strategy using PubMed for all the phase 3 trials in the last two decades evaluating survival outcome in MBC. We investigated the frequency of trials reporting survival outcome and response/resistance to treatment beyond progression. One hundred fifteen trials met our eligibility criteria: 69 (60 %) evaluated chemotherapy regimens (group A), 32 (28 %) evaluated targeted therapies (group B), and 14 (12 %) focused on endocrine treatment (group C). An OS benefit was demonstrated in approximately 22 % of the trials in each group. Less than 10 % of the trials in group A and B reported response data after progression on trial therapy. Post-progression treatment resistance was only reported in group A in 3 % (2/69) of the trials. In addition, the number of lines of treatment used post-progression was reported in 14 % (10/69), 9.4 % (3/32), and 14 % (2/14) of the trials in group A, B, and C, respectively. Post-progression survival and its effect on OS was reported in only 1 % (1/69), 3 % (1/32), and 7 % (1/14) of the trials for group A, B, and C respectively. A clear paucity of post-progression treatment information is noted in the majority of the phase 3 trials for MBC. We do know that OS can be affected partially or directly by treatments used after progression. In order to assess the true clinical benefit of a new drug and to have a complete evaluation of OS outcome, a detailed collection of post-progression treatment information is required and should be mandated in MBC trials.
Similar content being viewed by others


References
Ferlay J, Soerjomataram I, Ervik M et al. (2013) GLOBOCAN 2012 v1.0, Cancer incidence and mortality worldwide: IARC CancerBase No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer. Available from http://globocan.iarc.fr. Accessed 13 Dec 2013
Canadian Cancer Society’s Advisory Committee on Cancer Statistics (2013) Canadian cancer statistics 2013. Canadian Cancer Society, Toronto
Chia SK, Speers CH, D’yachkova Y et al (2007) The impact of new chemotherapeutic and hormone agents on survival in a population-based cohort of women with metastatic breast cancer. Cancer 110(5):973–979
Gennari A, Conte P, Rosso R et al (2005) Survival of metastatic breast carcinoma patients over a 20-year period: a retrospective analysis based on individual patient data from six consecutive studies. Cancer 104(8):1742–1750
Smith I (2006) Goals of treatment for patients with metastatic breast cancer. Semin Oncol 33(1 Suppl 2):S2–S5
Di Leo A, Bleiberg H, Buyse M (2003) Overall survival is not a realistic end point for clinical trials of new drugs in advanced solid tumors: a critical assessment based on recently reported phase III trials in colorectal and breast cancer. J Clin Oncol 21:2045–2047
Saad ED, Katz A (2009) Progression-free survival and time to progression as primary end points in advanced breast cancer: often used, sometimes loosely defined. Ann Oncol 20:460–464
Sherrill B, Hirst C, Wu Y et al (2007) Correlation between time to progression and overall survival in patients with metastatic breast cancer. In: 12th annual international meeting of the International Society for Pharmacoeconomics and Outcomes Research, 19–23 May 2007
Burzykowski T, Buyse M, Piccart-Gebhart MJ et al (2008) Evaluation of tumor response, disease control, progression-free survival, and time to progression as potential surrogate end points in metastatic breast cancer. J Clin Oncol 26:1987–1992
Miksad RA, Zietemann V, Gothe R et al (2008) Progression-free survival as a surrogate endpoint in advanced breast cancer. Int J Technol Assess Health Care 24:371–383
Cardoso F, Harbeck N, Fallowfield L (2012) Locally recurrent or metastatic breast cancer: ESMO clinical practice guidelines for diagnosis treatment and follow-up. Ann Oncol 23(Suppl 7):vii11–vii19
Andre F, Slimane K, Bachelot T et al (2004) Breast cancer with synchronous metastases: trends in survival during a 14-year period. J Clin Oncol 22(16):3302–3308
Mauri D, Polyzos NP, Salanti G et al (2008) Multiple-treatments meta-analysis of chemotherapy and targeted therapies in advanced breast cancer. J Natl Cancer Inst 100(24):1780–1791
Harris CA, Ward RL, Dobbins TA et al (2011) The efficacy of HER2-targeted therapy agents in metastatic breast cancer: a meta-analysis. Ann Oncol 22:1308–1317
Johnston SR (2011) The role of chemotherapy and targeted agents in patients with metastatic breast cancer. Eur J Cancer 47:38–47
Dean-Colomb W, Esteva FJ (2008) Her2-positive breast cancer: herceptin and beyond. Eur J Cancer 44:2806–2812
Kawalec P, Lopuch S, Mikrut A (2014) Effectiveness of targeted therapy in patients with previously untreated metastatic breast cancer: a systematic review and meta-analysis. Clin Breast Cancer pii:S1526-8209(14)00226-2 [Epub ahead of print]
Swain SM, Baselga J, Kim SB et al (2015) Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med 372(8):724–734
Jones SE (2008) Metastatic breast cancer: the treatment challenge. Clin Breast Cancer 8(3):224–233
Roché H, Vahdat LT (2011) Treatment of metastatic breast cancer: second line and beyond. Ann Oncol 22(5):1000–1010
Cardoso F, Di LA, Lohrisch C et al (2002) Second and subsequent lines of chemotherapy for metastatic breast cancer: what did we learn in the last two decades? Ann Oncol 13(2):197–207
Zhang XH, Giuliano M, Trivedi MV et al (2013) Metastasis dormancy in estrogen receptor-positive breast cancer. Clin Cancer Res 19(23):6389–6397
Saad ED, Katz A, Buyse M (2010) Overall survival and post-progression survival in advanced breast cancer: a review of recent randomized clinical trials. J Clin Oncol 28(11):1958–1962
Verma S, McLeod D, Batist G et al (2011) In the end what matters most? A review of clinical endpoints in advanced breast cancer. Oncologist 16(1):25–35
Wilcken N, Dear R (2008) Chemotherapy in metastatic breast cancer: a summary of all randomized trials reported 2000–2007. Eur J Cancer 44:2218–2225
Cheema PK, Burkes RL (2013) Overall survival should be the primary endpoint in clinical trials for advanced non-small-cell lung cancer. Curr Oncol 20(2):e150–e160
Korn EL, Freidlin B, Abrams JS (2011) Overall survival as the outcome for randomized clinical trials with effective subsequent therapies. J Clin Oncol 29(17):2439–2442
Kaufman B, Mackey JR, Clemens MR et al (2009) Trastuzumab plus anastrozole versus anastrozole alone for the treatment of postmenopausal women with human epidermal growth factor receptor 2-positive, hormone receptor-positive metastatic breast cancer: results from the randomized phase III TAnDEM Study. J Clin Oncol 27:5529–5537
Sparano JA, Vrdoljak E, Rixe O (2010) Randomized phase III trial of ixabepilone plus capecitabine versus capecitabine in patients with metastatic breast cancer previously treated with an anthracycline and a taxane. J Clin Oncol 28:3256–3263
Geyer CE, Forster J, Lindquist D et al (2006) Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med 355:2733–2743
Cortes J, O’Shaughnessy J, Loesch D et al (2011) Eribulin monotherapy versus treatment of physician’s choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet 377:914–923
Kaufman PA, Awada A, Twelves C et al (2015) Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline and a taxane. J Clin Oncol 33(6):594–601
Broglio KR, Berry DA (2009) Detecting an overall survival benefit that is derived from progression-free survival. J Natl Cancer Inst 101:1642–1649
Piccart M, Hortobagyi GN, Campone M et al (2014) Everolimus plus exemestane for hormone-receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: overall survival results from BOLERO-2. Ann Oncol 25(12):2357–2362
Tannock IF, Pond GR (2014) Everolimus, when combined with exemestane, adds toxicity with minimal benefit for women with breast cancer. Ann Oncol 25(10):2096. doi:10.1093/annonc/mdu371
Conflict of interest
S. Verma: Advisory Board—Roche, EISAI, Amgen, Novartis, Astra Zeneca. All remaining authors have declared no conflicts of interest.
Funding
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Raphael, J., Verma, S. Overall survival (OS) endpoint: an incomplete evaluation of metastatic breast cancer (MBC) treatment outcome. Breast Cancer Res Treat 150, 473–478 (2015). https://doi.org/10.1007/s10549-015-3342-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-015-3342-2