
Abstract
For more than a decade now blue native polyacrylamide gel electrophoresis (BN-PAGE) has been used for the study of the oxidative phosphorylation (OXPHOS) complexes. Catalytic activities of complexes I, II, IV and V can be assessed, after separation by gel electroforesis, by incubation of the BN-PAGE gel in specific staining solutions. However, until now, a reliable staining method for testing ubiquinol cytochrome c oxidoreductase (complex III) activity by BN-PAGE gel techniques was not available. In addition, spectrophotometric methods currently in use for detection of complex III deficiency in patients are not very sensitive. Here, we describe a newly developed diagnostic method for visualization of complex III activity by direct in-gel evaluation of ubiquinol cytochrome oxidoreductase activity. We validated the method by reporting the results in six patients with previously characterised complex III defects.
Similar content being viewed by others


Introduction
Complex III, ubiquinol:ferricytochrome-c oxidoreductase (EC 1.3.5.1), a transmembrane lipoprotein, is composed of ten nuclear and one mitochondrial encoded subunit (cytochrome b). The complex is located in the inner-mitochondrial membrane and transfers electrons from ubiquinol to cytochrome c. In a process, referred to as the Q-cycle, four protons are released into the inter-membrane space using four redox centres (cytochrome bL, cytochrome bH, cytochrome c1 and one iron sulphur cluster), passing two electrons to cytochrome c.
Defects in oxidative phosphorylation (OXPHOS) are not uncommon and very heterogeneous. Their incidence is estimated at 1 per 5000 live births (Schaefer et al. 2004). Only a limited number of patients with complex III deficiency have been reported. We can distinguish between three classes of complex III defects based on the underlying molecular defect: (1) mutations in a nuclear gene encoding an assembly protein for complex III (BCS1L) (OMIM 124000; de Lonlay et al. 2001), (2) mutations in a nuclear gene encoding a structural subunit of complex III (UQCRQ encoding subunit 7 (OMIM 61280; Barel et al. 2008)) and UQCRB encoding ubiquinol-cytochrome c reductase binding protein (OMIM 191330; Haut et al. 2003)), and (3) mtDNA alterations. Alterations in mtDNA leading to complex III deficiency have been found in the MT-CYB gene (OMIM 516020) encoding the cytochrome b and in the tRNA Tyr gene (Meulemans et al. 2007a, b). Mitochondrial DNA depletion can also cause complex III deficiency. The clinical phenotype of patients with complex III deficiency is variable with either skeletal muscle, heart muscle or brain being the predominantly affected organ (Benit et al. 2009). Exercise intolerance is the major presenting clinical symptom in most patients with a pathogenic mutation in MT-CYB, although the phenotype can vary (Blakely et al. 2005). Pathogenic mutations in the BCS1L gene result in decreased incorporation of the Rieske protein into the holo-complex and hence instability of the holo-complex. Patients with detrimental DNA alterations in the BCS1L gene share a phenotype characterised by low birth weight, proximal tubulopathy, hepatopathy and progressive neurological signs such as hypotonia, developmental delay and postnatal microcephaly (Benit et al. 2009). One specific mutation in BCS1L protein, p.S78G, is associated with GRACILE syndrome (Growth Retardation, Amino aciduria, Cholestasis, Iron overload, Lactic acidosis) (OMIM 603358; Visapää et al. 2002; Fellman et al. 2008). A milder phenotype also resulting from pathogenic alterations in the BSC1L gene is seen in the patients with Bjornstad’s syndrome, clinically characterised by sensorineural hearing loss and pili torti (OMIM 262000; Hinson et al. 2007).
The lack of sensitivity of currently used spectrophotometric assays might be a plausible explanation for the apparently low incidence of isolated complex III deficiency in patients. This was clearly illustrated in patients with mutations in the BCS1L assembly gene. The catalytic activity of complex III in these patients was only slightly decreased (Fellman 2002; De Meirleir et al. 2003) although BN-PAGE gel electrophoresis clearly demonstrated a decreased amount of protein in the complex (Kotarsky et al. 2010).
Earlier reports described the advantages of BN-PAGE techniques for detection of OXPHOS defects (Van Coster et al. 2001; Calvaruso et al. 2008; Díaz et al. 2009). One of several applications of this technique is BN-PAGE followed by in-gel activity staining, used for evaluation of the functional integrity of the individual OXPHOS complexes. Deficiencies of the complexes I, II, IV and V (EC 2.7.3.2, EC 1.6.5.3, EC 1.10.2.2 and EC 1.9.3.1) have been clearly demonstrated by this method in different tissues, including skeletal muscle, liver, heart muscle and cultured skin fibroblasts (Van Coster et al. 2001). However, complex III activity could not be evaluated thoroughly as no reliable staining method was available until now.
In 2006 we developed in our laboratory a new method for visualization of the catalytic activity of complex III in BN-PAGE gels. During the following years we optimised and validated this technique. Some results in patients with OXPHOS deficiencies were reported briefly in earlier papers (Meulemans et al. 2007a, b, Van Biervliet et al. 2009; van der Westhuizen et al. 2010; Kotarsky et al. 2010). In the paper presented here, we tried to highlight more clearly the usefulness of this technique for detection of complex III deficient patients.
Patients and methods
Patients
A variety of tissues from controls and patients was tested. Patients with documented complex III deficiencies were included in the study. This group consisted of patients with pathogenic mutations in BCS1L gene, in the mitochondrial tRNA Tyr gene, and with mtDNA depletion. The latter was either caused by mutations in the mtDNA polymerase gamma (EC 2.7.7.7) subunit 1 gene (POLG) or in the thymidine kinase 2 (EC 2.7.1.21) gene (TK2) (Table 1).
Methods
Ethics
For the specialised investigations described in this manuscript, ethical approval was obtained from Ghent University (UZGent nr 2005/075) and by the Committees of Medical Ethics at all collaborating institutions. Informed consents were obtained from the patients.
Sample preparation and electrophoresis
Isolation of mitochondria and separation of the OXPHOS complexes by BN-PAGE was performed as described earlier (Van Coster et al. 2001). In brief, mitochondria were prepared from patient and control tissues. These isolated mitochondria were solubilised and loaded in duplicate on the native gel. Approximately 30-60 μg mitochondrial protein from skeletal and heart muscle and 50-100 μg mitochondrial protein from liver were loaded on each lane. Following BN-PAGE separation, the first set of lanes was used for activity staining of complex I, III and IV and the second set of lanes was used to stain complex V and complex II. Maximum band density is reached within six hours of incubation. Five samples were simultaneously stained and processed in one BN-PAGE gel. In each gel a number of controls were included to assure good comparison of the signals between controls and patients.
Staining and interpretation
The activity staining of the complexes I, II, IV and V in the BN-PAGE gel was performed according to established protocols (Smet et al. 2005). For complex III activity staining a new method was developed. The major challenge consisted of finding a dye that interacts with the redox centra (heme) in complex III, and consequently precipitates in the gel. For this purpose an electron acceptor present in the staining kit from Pierce (1-StepTM TMB blotting, Pierce, Rockford, IL) was used. The kit is commercially available and is used for peroxidase based visualization of proteins in histochemical or immunoblotting assays. It also contains 3,3′,5,5′-tetramethylbenzidine (TMB), a peroxidase substrate, that functions as electron donor. In the presence of normally functioning heme groups in complex III, electrons are passed from the chromogenic substrate TMB to the electron acceptor present in the peroxide substrate buffer from the Pierce kit. As a result, a blue precipitate is produced in the direct environment of the complex III band. BN-PAGE gels were incubated for at least six hours in the staining solution and subsequently scanned in transmission mode using a GS-800 calibrated densitometer (Bio-Rad®). The resulting blue coloured band in the gel corresponding to complex III catalytic activity was evaluated by digital processing of the image in Adobe Photoshop® within the RGB working space created by Adobe Systems (1998). The Adobe RGB colour space is one of the most prominent colour modes in any graphic/photographic software. The name “RGB” is a reference to the three primary colours, Red, Blue and Green. In Adobe Photoshop®, RGB colour images are comprised of one composite channel and three grey scale channels containing the values of the three primary colours. In the option menu ‘curves’, a graphical representation of colour and light values is provided in a digital image. These values are displayed as a straight line which can be adjusted to alter particular colour and light values in the image. In ‘curves’ a particular colour channel can be chosen, in our study the blue channel, and its presence can be altered in the global image. Any upwards adjustment of the diagonal line in this channel will increase the blue colour, lowering of the line results in a more yellow colour. In this manner one can “extract” or lower the presence of the blue colour from the RGB image. The result is a shift towards a more green–yellow image. To maximise the visibility of precipitated TMB, the lower anchor point is moved horizontally to the left in the range between 180 and 230 (=input), causing a shift to more yellow in specific tonal regions of the image (Fig. 1a). The blue colour in the band produced by the coomassie dye coupled to complex V proteins stays unaltered. Using this procedure precipitated TMB in the band corresponding to the complex III activity becomes green-yellow and can easily be discriminated from the blue produced by coomassie coupled to proteins. After digital processing the intensity of the staining in the complex III bands can now be compared between patients and controls. To ensure accurate recording of images, calibration of the scanner is recommended with a grey card and colour chart card. Calibration is also recommended when more than one image capturing devise is used.

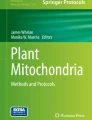
a. Complex III activity staining showing the effect of the subsequent digital processing: Complex III appears as a blue band following separation of the OXPHOS complexes by BN-PAGE and as a yellow-green band following activity staining and subsequent processing with Adobe Photoshop®. Left panel: prior to activity staining the complex III band stains blue due to the presence of coomassie blue bound to the protein in the complex. Middle panel: following the catalytic action of heme in complex III the TMB dye precipitates in the band corresponding to complex III (with the naked eye difficult to discriminate from the coomassie blue). Right panel: the blue colour of TMB shifts towards a yellow-green colour after processing the image with Adobe Photoshop® (‘curves’ – blue channel). Notice that the blue colour in the band corresponding to complex V did not shift towards green-yellow. b. Complex III activity staining in a lane containing the five OXPHOS complexes: Staining in the gel for complex III using TMB as electron donor. A lane loaded with solubilised mitochondria from control skeletal muscle contains all five OXPHOS complexes. Following activity staining for complex III, only the band corresponding to complex III changes into the yellow-green colour which demonstrates that the catalytic staining is specific for complex III. The left lane shows the bands prior to incubation with the specific staining solution. c. Complex III activity staining in controls and patients: Examples of in-gel staining following BN-PAGE separation in isolated mitochondria from different tissues obtained from controls and patients with selective genetic defects. In the patients P1, P2 and P5 equal loading was demonstrated by activity staining of complex I and IV in the same lane (data not shown). In the patient P3 equal loading was demonstrated by immunoblotting complex V using specific antibodies (data not shown). In the patients P4 and P6, equal loading could not be demonstrated by activity staining of complex I and IV in the same lane (these activities were also decreased as a result of mtDNA depletion). In these two patients, staining for complex II activity was performed using the same amount of mitochondrial proteins loaded on another lane. Complex II activity in the two patients was comparable with controls, confirming that the samples contained an equal amount of mitochondrial proteins (data not shown)
Results
In controls, activity staining of complex III produced in the BN-PAGE gel a sharp and prominent band with blue colour in the lanes loaded with mitochondria from heart or skeletal muscle. After digital processing, as described above, a shift to green-yellow is then induced. The intensity of the band was prominent in lanes loaded with mitochondria from heart and skeletal muscle but less prominent with mitochondria from liver. Only a faint band was produced in mitochondria isolated from cultured skin fibroblasts (data not shown). The activity staining is specific for complex III. The redox centres in the other four OXPHOS complexes do not interact with the substrate. Only the precipitate produced by complex III shifts to a yellow-green colour while the other bands remain blue (Fig. 1b).
In mitochondria isolated from heart and skeletal muscle from patients with pathogenic mutations in BCS1L gene, a reduced activity staining of complex III was seen in the BN-PAGE gel when compared to controls (patients 1, 2 and 3, Table 1, Fig. 1c). It was clear that the reduced activity staining resulted from a decreased amount of protein in the complex, which was already visible after separation of the complexes and before activity staining. Activity staining and amount of protein in the other OXPHOS complexes were normal. It is interesting to note that the catalytic activity of complex III assayed by spectrophotometric assay was not clearly reduced (Table 1).
In mitochondria isolated from skeletal muscle and liver from patients with mtDNA depletion (patients 4 and 6, Table 1), activity staining for complex III produced a decreased signal when compared to controls (Fig. 1c). Activity staining for complexes I and IV was also decreased, while the intensity of complex II activity staining was comparable to that found in controls (data not shown). In the BN-PAGE gel, before activity staining, a decrease of the amount of protein in complexes I, III and IV was visible due to the presence of coomassie blue coupled to the proteins in the gel (Fig. 1c).
The in-gel activity staining for complex III was decreased in skeletal muscle from a patient with pathogenic mutation in the tRNA Tyr gene (patient 5, Table 1). In this patient, the amount of protein in complex III was normal, as was the amount of protein in the other OXPHOS complexes. The findings in this patient show that the activity staining method allows detection of a defect in complex III, whilst the spectrophotometric assay had not revealed a clearly decreased catalytic activity.
Discussion
In this paper a newly developed method for in-gel activity staining of complex III is reported. A component in the buffer from a Pierce kit, developed for visualisation of histochemical and immunoblotting tests, is used as electron acceptor. 3,3′,5,5′-Tetramethylbenzidine (TMB) is utilised as electron donor for the heme groups in complex III. TMB is commonly used for activity staining of heme containing peroxidases (heterocyclic organic ring of porfyrines with an iron atom in the centre). Concomitant oxidation of TMB results in a colour shift. Pierce supplies two commercially available kits, one for ELISA (TMB remains in solution and can be used for spectrophotometric measurement but is not suitable to our purposes) and one for blotting purposes (TMB precipitates after oxidation).
Tissues from patients with documented defects in complex III were used to validate the sensitivity of the newly developed method. In tissues from six patients, a clear decrease of the band corresponding to complex III was seen following activity staining. In five of the six patients spectrophotometric analysis had shown normal or only slightly reduced catalytic activity (activities were within the interval of mean ± 3SD) (Table 1). From these results we can conclude that the new method for visualisation of complex III activity can be used as an alternative and sensible strategy for identification of patients with complex III deficiency.
One of the major challenges in the development of an activity staining method for complex III is the fact that the colour produced by oxidation of TMB is blue. Immediately after separation by BN-PAGE, proteins in the OXPHOS complexes are already visible in the gel as blue bands due to the presence of coomassie blue coupled to the proteins. The nature of the optimum wave lengths for oxidised TMB (370 nm and 652 nm) and coomassie blue (595 nm) makes the visualisation of the colour intensities difficult for the human eye. In the ELISA applications for TMB, this problem is circumvented by adding acid which stops the enzyme reactions and converts the blue colour to yellow that absorbs at 450 nm. We investigated the application of 2 M hydrochloric acid and found that the blue colour indeed shifted to yellow. However, within seconds of the colour shift, the yellow precipitate started to dissolve and the yellow band faded away. This is probably what Zerbetto and co-workers had experienced (Zerbetto et al. 1997). We therefore preferred digital processing of the blue colour using ‘curves’ in Adobe photoshop®. The coomassie bands remain blue while the blue purple colour from oxidised TMB changes to a yellow-green. An alternative way to avoid interference of the coomassie dye is the use of high resolution clear native electrophoresis (hrCNE) as described by Wittig and co-workers (Wittig et al. 2007). In this method the coomassie dye is neither added to the cathodal buffer, nor to the solubilised mitochondria prior to electrophoresis. Instead a non-coloured mixture of anionic and neutral detergents is used. Unfortunately, successful in-gel activity staining of all OXPHOS complexes except for complex III was achieved following the use of the hrCNE-1 technique (data not shown).
For quantification of OXPHOS complexes activities, spectrophotometric enzymatic assays remain the ‘golden standard’ (Benit et al. 2006). These assays produce reliable results for complexes with relatively low inhibitor insensitive fraction (i.e. complex IV). However, for complexes with a high inhibitor resistant fraction the sensitivity of the assays is too low. This is clearly the case for the spectrophotometric complex III assay where antimycin A is used as inhibitor. The antimycin A insensitive fraction is even higher than the antimycin A sensitive fraction which explains the variable results and the large standard deviation of this spectrophotometric assay (Luo et al. 2008). The problem of the high inhibitor resistant fraction can be circumvented by the use of BN-PAGE techniques. In these gels, only large protein complexes with molecular weights between 200 and 800 kDa are retained, while enzymes with smaller size responsible for most of the inhibitor resistant activity are absent.
One of the major disadvantages of the method is that it is not quantitative. Quantification of the bands in the BN-PAGE gel using densitometry is hard to accomplish. The coomassie dye attached to the protein is responsible for a blue colour which makes quantification of the precipitate produced by the enzymatic conversion difficult. Reliable detection of deficient complex activity is ensured by selecting tissue specific controls with comparable activities of the other non-deficient OXPHOS complexes. In our experiments the difference between the normal activities and the deficient activities in the patients was so obvious that densitometric evaluation was not performed. Finally, only severely deficient OXPHOS activities are thought to be of clinical significance.
Another disadvantage of the method described here is the fact that a component of the buffer from the Pierce kit is used as electron acceptor. A laboratory made solution containing this component would make the method more generic. The manufacturer does not disclose the components of the buffer solution for the Pierce kit. We tried to use other solutions as electron acceptor (e.g. cytochrome c) but were not successful.
In summary, we have clearly demonstrated that complex III activity can be visualised in a BN-PAGE gel using mitochondria from skeletal muscle and liver. This newly developed in-gel activity staining procedure serves as a powerful strategy for detection of patients with complex III deficiency not identified by classic enzymatic activity measurements of ubiquinol cytochrome c oxidoreductase.
Abbreviations
- BCS1L :
-
Human bc1 synthesis like gene
- BN-PAGE:
-
Blue native polyacrylamide gel electrophoresis
- hrCNE:
-
High resolution Clear Native Electrophoresis
- mtDNA:
-
Mitochondrial DNA
- OXPHOS:
-
Oxidative phosphorylation
- POLG :
-
Gene coding for polymerase gamma
- TK2 :
-
Thymidine kinase gene
- TMB:
-
3,3′,5,5′-tetramethylbenzidine
- UQCRB:
-
Ubiquinol-cytochrome c reductase binding protein
References
Barel O, Shorer Z, Flusser H et al (2008) Mitochondrial complex III deficiency associated with a homozygous mutation in UQCRQ. Am J Hum Genet 82:1211–1216
Blakely EL, Mitchell AL, Fisher N et al (2005) A mitochondrial cytochrome b mutation causing severe respiratory chain enzyme deficiency in humans and yeast. FEBS J 272:3583–3592
Calvaruso MA, Smeitink J, Nijtmans L (2008) Electrophoresis techniques to investigate defects in oxidative phosphorylation. Methods 46:281–287
Benit P, Goncalves S, Philippe Dassa E et al (2006) Three spectrophotometric assays for the measurement of the five respiratory chain complexes in minuscule biological samples. Clin Chim Acta 374:81–86
Benit P, Lebon S, Rustin P (2009) Respiratory-chain diseases related to complex III deficiency. Biochim Biophys Acta 1793:181–185
de Lonlay P, Valnot I, Barrientos A et al (2001) A mutant mitochondrial respiratory chain assembly protein causes complex III deficiency in patients with tubulopathy, encephalopathy and liver failure. Nat Genet 29:57–60
De Meirleir L, Seneca S, Damis E et al (2003) Clinical and diagnostic characteristics of complex III deficiency due to mutations in the BCS1L gene. Am J Med Genet A 121A:126–131
Díaz F, Barrientos A, Fontanesi F (2009) Evaluation of the mitochondrial respiratory chain and oxidative phosphorylation system using blue native gel electrophoresis. Curr Protoc Hum Genet. 19:19.4
Fellman V (2002) The GRACILE syndrome, a neonatal lethal metabolic disorder with iron overload. Blood Cells Mol Dis 29:444–450
Fellman V, Lemmelä S, Sajantila A, Pihko H, Järvelä I (2008) Screening of BCS1L mutations in severe neonatal disorders suspicious for mitochondrial cause. J Hum Genet 53:554–558
Haut S, Brivet M, Touat G et al (2003) A deletion in the human QP-C gene causes a complex III deficiency resulting in hypoglycaemia and lactic acidosis. Hum Genet 113:118–122
Hinson JT, Fantin VR, Schonberger J et al (2007) Missense mutations in the BCS1L gene as a cause of the Bjornstad syndrome. N Engl J Med 356:809–819
Kotarsky H, Karikoski R, Mörgelin M et al (2010) Characterization of complex III deficiency and liver dysfunction in GRACILE syndrome caused by a BCS1L mutation. Mitochondrion 10:497–509
Luo C, Long J, Liu J (2008) An improved spectrophotometric method for a more specific and accurate assay of mitochondrial complex III activity. Clin Chim Acta 395:38–41
Meulemans A, Seneca S, Smet J et al (2007a) A new family with the mitochondrial tRNAGLU gene mutation m.14709 T > C presenting with hydrops fetalis. Eur J Paediatr Neurol 11:17–20
Meulemans A, De Paepe B, De Bleecker J et al (2007b) Two novel mitochondrial DNA mutations in muscle tissue of a patient with limb-girdle myopathy. Arch Neurol 64:1339–1343
Schaefer AM, Taylor RW, Turnbull DM, Chinnery PF (2004) The epidemiology of mitochondrial disorders–past, present and future. Biochim Biophys Acta 1659:115–120
Smet J, Devreese B, van Beeumen J, Van Coster R (2005) Nondenaturing polyacrylamide gel electrophoresis as a method for studying protein interactions: applications in the analysis of mitochondrial OXPHOS complexes. In: Celis JE (ed) Cell biology: a laboratory handbook. Academic, San Diego, pp 259–264
Van Biervliet S, Verloo P, Vande Veldel S et al (2009) Abdominal pain and vomiting as first sign of mitochondrial disease. Acta Gastroenterol Belg 72:365–368
van der Westhuizen FH, Smet J, Levanets O et al (2010) Aberrant synthesis of ATP synthase resulting from a novel deletion in mitochondrial DNA in an African patient with progressive external ophthalmoplegia. J Inherit Metab Dis 2010 Jan 16 [Epub ahead of print]
Van Coster R, Smet J, George E et al (2001) Blue native polyacrylamide gel electrophoresis: a powerful tool in diagnosis of oxidative phosphorylation defects. Pediatr Res 50:658–665
Visapää I, Fellman V, Vesa J et al (2002) GRACILE syndrome, a lethal metabolic disorder with iron overload, is caused by a point mutation in BCS1L. Am J Hum Genet 71:863–876
Wittig I, Karas M, Schägger H (2007) High resolution clear native electrophoresis for in-gel functional assays and fluorescence studies of membrane protein complexes. Mol Cell Proteomics 6:1215–1225
Zerbetto E, Vergani L, Dabbeni-Sala F (1997) Quantification of muscle mitochondrial oxidative phosphorylation enzymes via histochemical staining of blue native polyacrylamide gels. Electrophoresis 18:2059–2064
Acknowledgments
We thank Mr Christophe Meul, professor in Integrated Digital Techniques and Fine Arts, for his help in Photoshop® for digital processing of images. We also thank Mary Phelan for her help with correcting the English language. This study was supported by a grant from the Fund for Scientific Research Belgium (FWO), contract grant number G.0666.06 (Universiteit Gent and Vrije Universiteit Brussel) and from ‘KidAuQuai’, Ghent, Belgium, and the Medical Society of Finland (Finska Läkaresällskapet).
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by: John Christodoulou.
References to electronic databases: Mitochondrial complex III deficiency: OMIM 124000. UQCRQ encoding subunit 7: OMIM 61280. UQCRB encoding ubiquinol-cytochrome c reductase binding protein: OMIM 191330. Cytochrome b of Complex IIII, MTCYB: OMIM 516020. GRACILE syndrome (Growth retardation, Amino aciduria, Cholestasis, Iron overload, Lactic acidosis): OMIM 603358. Bjornstad syndrome: OMIM 262000. NADH:ubiquinone oxidoreductase (complex I): EC 1.6.5.3. Succinate:ubiquinone oxidoreductase (complex II): EC 1.3.5.1. Ubiquinol:ferricytochrome-c oxidoreductase (complex III): EC 1.10.2.2. Ferrocytochrome-c:oxygen oxidoreductase (complex IV): EC 1.9.3.1. ATP phosphohydrolase (complex V): EC 3.6.1.3. Deoxynucleoside-triphosphate:DNA deoxynucleotidyltransferase (DNA-directed; DNA polymerase gamma): EC 2.7.7.7. Mitochondrial thymidine kinase 2: EC 2.7.1.21.
Competing of interest: None declared.
Rights and permissions
About this article
Cite this article
Smet, J., De Paepe, B., Seneca, S. et al. Complex III staining in blue native polyacrylamide gels. J Inherit Metab Dis 34, 741–747 (2011). https://doi.org/10.1007/s10545-011-9315-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10545-011-9315-7