
Abstract
It is considered to be normal practice to close laparoscopy trocar incision sites with skin sutures. We could not find evidence to show this had been validated by a clinical trial. The aim of this study was to assess the need for sutures from both a clinical and cosmetic point of view. Fifty female patients undergoing laparoscopy were randomly allocated into suture and non-suture groups. Patients were reviewed at 1 and 6 weeks. Using a visual analogue scale, a number of parameters including bleeding, bruising, infection and pain were evaluated. Results were recorded from the observer and the patient. Additional data regarding patients' satisfaction were also collected. These results were then analysed. After analysis, no statistical difference was demonstrated between the two groups for bleeding, bruising, infection or pain. Both groups were equally satisfied with their procedures and the cosmetic appearance of the scar at 6 weeks. They spent a similar time off work. The majority (59.1 %) of patients would prefer not to have sutures for subsequent laparoscopy. Conclusion: Laparoscopic incisions, which have haemostasis, do not require skin sutures either clinically or for cosmesis.
Similar content being viewed by others

Introduction
Laparoscopic surgery is now a commonplace procedure [1]. It has become the accepted, if not the preferred, approach to a wide range of gynaecological pathologies. Further innovative advances continue to broaden its field and potential.
Through clinical observation, it was felt that suturing laparoscopic incisions was causing postoperative problems such as infection and irritation. After a literature search, we concluded that there was little or no evidence to support the clinical need to suture the incisions.
The aim of this study was to evaluate the current practice of suturing trocar incision sites. Cosmetic and clinical outcomes were compared to a control group.
Methods
The study took place in the Department of Obstetrics and Gynaecology in the Queens Medical Centre, Nottingham, England. All subjects were undergoing either diagnostic laparoscopy or laparoscopic sterilisation on a day case unit. A consultant gynaecologist performed all procedures. Ten-millimetre vertical umbilical port and 5-mm suprapubic port incisions were made in all cases.
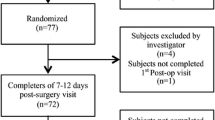
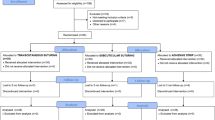
Fifty-two patients aged 25 to 64 years (mean, 42.5 years) with a mean BMI of 26.6 presenting consecutively to routine lists were considered. Patients who did not require a suture for haemostasis were alternately allocated into suture and non-suture groups. Two patients had to be excluded, as they needed to be sutured to achieve haemostasis, leaving a total of 50. 2/0 Vicryl rapide sutures were used to the incision in the suture group; a simple sterile dressing was used in the non-suture group.
A single observer then assessed patients at 1 and 6 weeks post procedure. Using a visual analogue scale, both the patient and observer evaluated bruising, pain, bleeding, cosmetic effect and overall satisfaction. Other information was also collected to assess post-op morbidity. The results were then tabulated and analysed. Data were tested using Student's t test.
Results
After statistical examination, patients' results showed no significant difference in the level of bruising, bleeding, pain or infection between the two groups, when questioned at 1 week. One non-suture patient reported bleeding on the second postoperative day, from the incision site; this stopped with pressure and did not require medical intervention. These results were mirrored in the clinical observer's findings at 1 week. See Table 1.
When the patients were reassessed at 6 weeks, no difference was noted between the groups for cosmetic outcome. The average time taken to return to work was 7.73 days, with no significant difference between the two groups. Patients' satisfaction post procedure did not seem to relate to the presence or absence of sutures.
The suture took an average of 23.7 days to drop out. Some patients removed their own sutures, and one patient still had the suture in place at her 6-week check. See Table 2.
Of the patients in the suture group, 30.7 % would have preferred no suture. In the non-suture group, 87.5 % would be happy for future laparoscopy incisions of a similar size to be left open. Although no statistical differences were seen, 59.1 % of the patients overall would prefer incisions not to be sutured in future laparoscopies.
Discussion
The results show there were no significant differences between the two groups on any of the outcome parameters. Postoperative morbidity and cosmetic outcome were the same irrespective of whether a suture was used. Despite literature searches, we were unable to find any other gynaecological studies to directly compare our results with.
A recent trial compared paper tape with conventional sutures for skin closure after colorectal surgery. Their findings suggested paper tape to be quicker, with improved patient satisfaction and no associated increase in wound infection [2]. Tissue glue has also been considered for the closure of port sites; a review article showed it to be effective and well tolerated for haemostasis and wound healing [3].
As our practices become increasingly dependent on evidence-based medicine, we must begin to justify even the most minor procedures through clinical trial. This is a small group, and increasing the sample size may bring out statistic differences between the two groups.
To date there seems to be no obvious benefit in suturing the trocar incision ports. Not suturing has now become our practise on this consultant firm. Additional clinical studies with a larger number of patients are required to confirm these potential benefits.
Conclusion
Laparoscopic trocar skin incisions, which have haemostasis at the time of operation, do not require skin sutures either for clinical or cosmetic benefit. Importantly, patient preference was against suturing.
References
Cheong YC, Wang TM, Tucker D, Li TC, Cooke ID (2001) The changing nature of elective laparoscopic surgery. Hum Fertil 4(1):31–36
Chen HH et al (2001) Prospective study comparing wounds closed with tape to sutured wounds in colorectal surgery. Arch Surg 136(7):801–803
Dunn CJ, Goa KL (1999) Fibrin sealant: a review of its use in surgery and endoscopy. Drugs 58(5):863–866
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Crossley, S., Houda, M. & Powell, M. Prospective observational study to evaluate the need for skin sutures to close laparoscopic skin incisions. Gynecol Surg 9, 411–413 (2012). https://doi.org/10.1007/s10397-012-0750-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10397-012-0750-8