
Abstract
Angiomyomas of the uterus are uncommon tumors that apparently arise from the smooth muscles of blood vessels. We describe here an unusually large angiomyoma of the uterus in a 45-year-old woman who presented with an abdominal lump. An exploratory laparotomy was followed by a pan-hysterectomy. The dissected section of the uterus showed a huge fleshy mass measuring 20 cm with areas of hemorrhage. Histopathological examination showed many dilated vascular spaces amidst smooth muscle bundles, which is characteristic of cavernous angiomyoma of the uterus.
Similar content being viewed by others


Introduction
Leiomyomas are common tumors found in the uterus and are present in 25% of women of reproductive age [1]. Incidence rates of more than 80% have been reported in asymptomatic women evaluated by ultrasound examination [2]. Angiomyomas of the uterus are uncommon tumors, and only a few cases have been reported in literature [3–9]. Most cases were diagnosed after surgery, and the majority were small in size. We describe here an unusually large angiomyoma of the uterus.
Case report
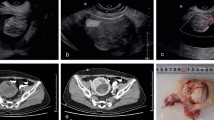
A 45-year-old multiparous woman presented in May 2006 with an abdominal lump of 6 months duration. Her cycles were regular and there was no menorrhagia. There were no other significant symptoms, including any history of weight loss. On examination, there was a large mass arising from the pelvis, corresponding to 32 weeks gestation. Internal examination revealed that the cervix was drawn up and the uterus could not be felt separate from the mass. Clinically an ovarian pathology could not be excluded. On rectal examination, the rectal mucosa was normal and there were no palpable nodules in the pouch of Douglas. Hematological and biochemical investigations were normal. Pap smear was normal. An ultrasound of the abdomen and pelvis revealed a mass extending up to the epigastrium with solid and hyperechoic areas. The ovaries were not visualized separately. The upper abdomen was normal. Upper gastro-intestinal endoscopy and chest roentgenogram were normal.
With the provisional diagnosis of an ovarian tumor, an exploratory laparotomy was performed. The mass was found to be arising from the uterus, which was soft, vascular and enlarged to 30 × 22 × 21 cm. The tumor extended in to the right broad ligament. Both the ovaries and tubes were normal. Examination of the upper abdomen was unremarkable and there was no lymphadenopathy. Peritoneal washings were collected, a total hysterectomy with bilateral salpingo-oophorectomy was performed, and the specimen weighing 5.1 kg was removed. When the enlarged uterus was cut open, it contained about 2 l of blood. Two units of packed cells were transfused to replace intra-operative blood loss. The postoperative period was uneventful, and the patient was discharged on the 10th day after surgery.
Cytological examination of the peritoneal washings was negative for malignant cells. On gross examination, the uterus was asymmetrically enlarged and the endometrial cavity was pushed to one side (Fig. 1). The myometrium showed a huge fleshy mass measuring 20 cm with areas of hemorrhage. Histopathological examination revealed secretory phase endometrium with foci of adenomyosis in the myometrium. Multiple sections taken from the fleshy mass showed many dilated vascular spaces amidst smooth muscle bundles (Fig. 2, 3), which is characteristic of cavernous angiomyoma of the uterus. There was no atypia, necrosis or increased mitotic figures. The cervix and ovaries were normal.

Gross appearance of the uterus

Prominent vessels interspersed with smooth muscle (HE, 100×)

Vascular spaces surrounded by myometrial tissue (HE, 200×)
Discussion
Leiomyomas are smooth muscle tumors that are generally well differentiated. They exhibit interlacing fascicles of uniform spindle cells with elongated nuclei that have blunt ends [10]. Angiomyomas are also described as vascular leiomyomas and angioleiomyomas. They are leiomyomas that apparently arise from the smooth muscles of blood vessels. In contrast to leiomyomas, angioleiomyomas contain many dilated vascular spaces amidst smooth muscle bundles arranged in a more concentric fashion. These vascular spaces are lined with an endothelium [11]. Angioleiomyomas are well circumscribed or encapsulated and contain minimal collagen. In addition, larger angioleiomyomas frequently have areas of mucinous alteration.
The three histologic subtypes of angioleiomyomas based on differences in the vascular channels are solid or capillary, cavernous, and venous. The solid or capillary type contains many small vascular spaces. Cavernous tumors have dilated vascular spaces with only small amounts of smooth muscle. The venous subtypes contain veins with thick muscular walls [12].
Various abnormal karyotypes in cases of leiomyomas have been described [13]. Hennig et al. [8] described clonal karyotypic alterations of a uterine angioleiomyoma that had not been reported in uterine smooth muscle tumors before.
Angiomyomas have been described in various organs of the body, though mostly in the lower extremities [14]. Angiomyomas of the genital tract are rare; those described in literature are mainly those involving the uterus and one report involving the ovary [15].
In the previously reported cases, patients have presented with symptoms of abnormal uterine bleeding [5, 6], palpable abdominal mass [6], pain in the abdomen [4], and pressure symptoms [3]. Most tumors were small in size; an unusually large angiomyoma similar to the one here has been described only by Hsieh et al. [6].
Pre-operative imaging of the tumor has been described. Agorastos et al. [5] described a multicystic pelvic mass on ultrasound that they mistook for an ovarian pathology. Hsieh et al. [6] described a heterogeneously multilobulate mass with solid and laminated configuration, with cystic and multiseptal components on computed tomography.
The treatment of angiomyomas, both uterine and extra-uterine, is complete surgical excision of the tumor. In cases involving the uterus, either hysterectomy or excision of the tumor may be performed. Outcomes with both the treatment modalities are good.
References
Vollenhoven BJ, Lawrence AS, Healy DL (1990) Uterine fibroids: a clinical review. Br J Obstet Gynaecol 97:285–298
Day Baird D, Dunson DB, Hill MC, Cousins D, Schectman JM (2003) High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol 188:100–107
Konichezky M, Reif R, Bulovsky I (1980) Benign angiomyoma of the uterus with unusual macroscopic appearance. Int J Gynaecol Obstet 18:4–6
Jameson CF (1990) Angiomyoma of the uterus in a patient with tuberous sclerosis. Histopathology 16:202–203
Agorastos T, Dinas K, Patsiaoura K (2001) Cystic degenerated angioleiomyoma mimicking ovarian pathology. Acta Obstet Gynecol Scand 80:863
Hsieh CH, Lui CC, Huang SC, Ou YC, Chang Chien CC, Lan KC, Huang KH (2003) Multiple uterine angioleiomyomas in a woman presenting with severe menorrhagia. Gynaecol Oncol 90:348–352
Gyure KA, Hart WR, Kennedy AW (1995) Lymphangiomatosis of the uterus associated with tuberous sclerosis and malignant neoplasia of the female genital tract: a report of two cases. Int J Gynecol Pathol 14:344–351
Hennig Y, Caselitz J, Stern C, Bartnitzke S, Bullerdiek J (1999) Karyotype evolution in a case of uterine angioleiomyoma. Cancer Genet Cytogenet 108:79–80
Prabha V, Kumari SS, Subbarao TU, Jeevan D, Bagyalakshmi KR, Kumar PN, Mohan VP (2002) Angiomyoma/angioleiomyoma of the uterus: a rare and unusual presentation. Antiseptic 99:284–285
Robboy SJ, Kurman RJ, Merino MJ (2005) The female reproductive system. In: Rubin E (Ed) Rubin’s pathology: clinicopathological foundations of medicine, 4th edn. Lippincott, Williams and Wilkins, Philadelphia pp. 926–995
Weiss SW, Goldblum JR (eds) (2001) Enzinger and Weiss’s: soft tissue tumors. 4th edn. Mosby, St. Louis
Katenkamp D, Kosmehl H, Langbein L (1988) Angiomyoma. Eine pathologo-anatomische Analyse von 229 Fällen. Zentralbl Allg Pathol 134:423–433
Lobel MK, Somasundaram P, Morton CC (2006) The genetic heterogeneity of uterine leiomyomata. Obstet Gynecol Clin North Am 33:13–39
Hachisuga T, Hashimoto H, Enjoji M (1984) Angioleiomyoma: a clinicopathological reappraisal of 562 cases. Cancer 54:126–130
Vicari AM, Sabiene A, Taccagni G, Luoni R, Carlucci M, Pozza G (1986) Sclerosi tuberose: segnalazione di un caso peculiare. Recenti Prog Med 77:466–469
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koshy, A.K., Chaturvedula, L., Habeebullah, S. et al. Angiomyoma of the uterus: case report and review of literature. Gynecol Surg 5, 169–171 (2008). https://doi.org/10.1007/s10397-007-0352-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10397-007-0352-z