
Abstract
Objective
The aim of the work was to compare the dosimetric results that were obtained by using two treatment planning systems (TPS) Siemens KonRad version 2.2.23, Elekta XiO version 4.4 to perform a simultaneous integrated boost (SIB) for head and neck and central nervous system (CNS) cases in paediatric patients.
Methods
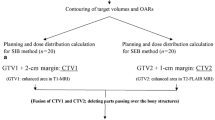
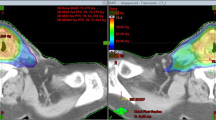
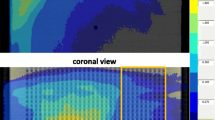
The CT scan data for five paediatric patients, with head and neck and CNS tumors, were transferred into both of the TPSs. Clinical step-and-shoot intensity-modulated radiotherapy (IMRT) treatment plans were designed using 6 MV photon beam for delivery on a Siemens Oncor Accelerator with multileaf collimator MLC (82 leaf). Plans were optimized to achieve the same clinical objectives using the same beam energy, number and direction of beams. The analysis was based on isodose distributions, the dose volume histogram (DVH) for planning target volume (PTV) and the relevant organs at risk (OARs) as well as volume receiving 2 Gy and 5 Gy, also total number of segments, MU/segment, and the number of MU/cGy had been investigated. Treatment delivery time and conformation number were two other parameters in this study.
Results
The segmentation using KonRad was more efficient, resulting in fewer segments (reduction between 13.2% and 48.3%), fewer MUs (reduction between 10.7% and 33%) and that reflected on treatment delivery times to be shorter by up to 8 min or 46%. In most of the cases KonRad had the highest volume receiving in excess of 2 and 5 Gy, and XiO showed the lowest. Also KonRad achieved slightly better conformality (0.76 ± 0.054) than XiO (0.73 ± 0.05) while XiO presented a higher modulation factor value (3.3 MU/cGy) than KonRad (2.4 MU/cGy).
Conclusion
The KonRad treatment planning system was found to be superior to the XiO treatment planning system. This is true for the possible increase of radiation-induced secondary malignancies as well as for the local control.
Similar content being viewed by others
References
AAPM report No. 13. Physical aspects of quality assurance in radiation therapy. New York: American Institute of Physics, 1983.
Fraass B, Doppke K, Hunt M, et al. American Association of Physicists in Medicine Radiation Therapy Committee Task Group 53: quality assurance for clinical radiotherapy treatment planning. Med Phys, 1998, 25: 1773–1829.
Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys, 1991, 21: 109–122.
Milano MT, Constine LS, Okunieff P. Normal tissue tolerance dose metrics for radiation therapy of major organs. Semin Radiat Oncol, 2007, 17: 131–140.
Stein J, Mohan R, Wang XH, et al. Number and orientations of beams in intensity-modulated radiation treatments. Med Phys, 1997, 24: 149–160.
Verhey LJ. Comparison of three-dimensional conformal radiation therapy and intensity-modulated radiation therapy systems. Semin Radiat Oncol, 1999, 9: 78–98.
Dai J, Zhu Y. Minimizing the number of segments in a delivery sequence for intensity-modulated radiation therapy with a multileaf collimator. Med Phys, 2001, 28: 2113–2120.
Van’t Riet A, Mak AC, Moerland MA, et al. A conformation number to quantify the degree of conformality in brachytherapy and external beam irradiation: application to the prostate. Int J Radiat Oncol Biol Phys, 1997, 37: 731–736.
Both S, Alecu IM, Stan AR, et al. A study to establish reasonable action limits for patient-specific quality assurance in intensity-modulated radiation therapy. J Appl Clin Med Phys, 2007, 8: 1–8.
Dong L, Antolak J, Salehpour M, et al. Patient-specific point dose measurement for IMRT monitor unit verification. Int J Radiat Oncol Biol Phys, 2003, 56: 867–877.
Leybovich LB, Sethi A, Dogan N. Comparison of ionization chambers of various volumes for IMRT absolute dose verification. Med Phys, 2003, 30: 119–123.
Xing L, Li JG. Computer verification of fluence map for intensity modulated radiation therapy. Med Phys, 2000, 27: 2084–2092.
Jursinic PA, Nelms BE. A 2-D diode array and analysis software for verification of intensity modulated radiation therapy delivery. Med Phys, 2003, 30: 870–879.
Hall EJ, Wuu CS. Radiation-induced second cancer: the impact of 3D-CRT and IMRT. Int J Radiat Oncol Biol Phys, 2003, 56: 83–88.
Hall EJ. Intensity-modulated radiation therapy, protons, and the risk of second cancers. Int J Radiat Oncol Biol Phys, 2006, 65: 1–7.
Fogliata A, Nicolini G, Alber M, et al. On the performances of different IMRT Treatment Planning Systems for selected paediatric cases. Radiat Oncol, 2007, 2: 7.
Van Dyk J, Barnett RB, Cygler JE, et al. Commissioning and quality assurance of treatment planning computers. Int J Radiat Oncol Biol Phys, 1993, 26: 261–273.
Studer G, Huguenin PU, Davis JB, et al. IMRT using simultaneously integrated boost (SIB) in head and neck cancer patients. Radiat Oncol, 2006, 1: 7.
Teh BS, Mai WY, Grant WH 3rd, et al. Intensity modulated radiotherapy (IMRT) decreases treatment-related morbidity and potentially enhances tumor control. Cancer Invest, 2002, 20: 437–451.
Reitz B, Miften M. Comparison of the KonRad IMRT and XiO treatment planning systems. J Appl Clin Med Phys, 2008, 9: 2770.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Attalla, E.M., Eldesoky, I. & Eldebawy, E. Simultaneous integrated boost IMRT in pediatric: evaluation for two commercial treatment planning systems. Chin. -Ger. J. Clin. Oncol. 12, 6–14 (2013). https://doi.org/10.1007/s10330-012-1083-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10330-012-1083-9