
Abstract
This cost-of-illness analysis is part of a Europe-wide study on the costs of multiple sclerosis (MS) and is based on information from patients in Austria. The objective was to estimate the costs and quality of life (QOL) related to the level of disease severity and progression. Questionnaires were sent to 2995 patients registered with a nationwide patient organization. Patients were asked to provide details regarding the type of disease, relapses, level of functional disability, resource consumption (medical and non-medical), work absence, sick leave and informal care, as well as QOL. Surveys from a total of 1.019 (34.0%) patients were used in the analysis, of which the mean (standard deviation [SD]) age was 50 (12.2) years; 70% of patients were female. Patients with mild disease (Expanded Disability Status Scale [EDSS] score 0–3) represented 41% of patients, 36% had moderate disease (EDSS score 4–6.5) and 22% had severe disease (EDSS score ≥7). The mean (SD) EDSS score in the sample was 4.4 (2.4), with a mean (SD) utility of 0.55 (0.32).
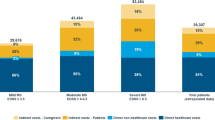
Costs are presented from the societal perspective as well as from the viewpoint of payers of care and invalidity. Mean total annual costs for an average patient in the sample were estimated at € 40.300 in the societal perspective, whereas payers’ costs were estimated at only half of this. Disease-modifying drugs represented a quarter of all costs in the payer perspective, but only 12% of societal costs. For society, the highest cost was the loss of productivity (36%), while payments for this loss (invalidity pensions and sick-leave compensation) accounted for only 21% of total costs to payers. Costs are highly correlated with disease progression, increasing four-fold from early disease to very severe disease (€ 16.000 to € 63.800). Mean annual costs per patient reported are thus determined by the distribution of disease severity in the sample. Workforce participation decreases from roughly 75% in early disease to less than 10% in the late stages, despite the fact that 70% of patients with an EDSS score of 8 or 9 are still below the official retirement age. Consequently, productivity losses increase over fivefold. In parallel, costs of informal care increase from € 325 per year at an EDSS score of 0–1 to over € 20.000 at an EDSS score of 8–9. Hospitalization is very infrequent in early disease, representing less than € 1.000 for patients with an EDSS score of 0–1, but increases steeply for patients with an EDSS score ≥5. QOL, measured as utility scores, decreases rapidly from almost 0.90 to 0.05 as disability becomes severe. However, the loss of utility is evident at all disease levels. Young patients with an EDSS score of approximately 2 have a utility that is 0.15 lower than matched individuals from the general population. This loss increases to approximately 0.4 for patients over 60 years of age with an average EDSS score of 6.0–6.5. Patients with a recent relapse had lower utility (–0.1) and higher costs (+ € 4.750).






Similar content being viewed by others


References
Kobelt G, Berg J, Lindgren P, Fredrikson S, Jönsson B (2006) Costs and quality of life of multiple sclerosis in Europe. J Neurol Neurosurg Psychiatry. Published online 11 May 2006
Ganzinger U, Badelt C, Vass K et al. (2004) Krankheitskosten der multiplen Sklerose in Österreich. Querschnittstudie unter Brücksichtigung der Lebensqualität, Der Nervenarzt
Baumhackl U, Eibl G, Ganzinger U et al. (2002) Prevalence of multiple sclerosis in Austria. Results of a nationwide survey. Neuroepidemiology 21: 226–234
Pugliatti M, Rosati R, Carton H et al. (2006) The prevalence and incidence of multiple sclerosis in Europe. Eur J Neurol 13: 1–23
Kurtzke J (1983) Rating neurological impairment in multiple sclerosis and expanded disability status scale (EDSS). Neurology 33: 1444–1452
The EuroQol Group (1990) EuroQol – a new facility for the measurement of health-related quality of life. Health Policy 16: 199–208
Dolan P (1995) A social tariff for EuroQol: results from a UK general population survey. Centre for Health Economics, University of York: York
Eichler H, Kong S, Gerth W, Al E (2004) Use of cost-effectiveness analysis in health care resource allocation decision-making: how are cost-effectiveness thresholds expected to emerge? Val Health 7: 518–528
Kobelt G (2004) Economic evidence in multiple sclerosis: a review. Eur J Health Econ 5: 54–62
Kobelt G, Lindgren P, Parkin D, Jönsson B (2000) Costs and quality of life in multiple sclerosis. A cross-sectional observational study in the United Kingdom. SEE/EFI Working Paper Series in Economics and Finance No. 399. Stockholm School of Economics; Stockholm, Sweden
Henriksson F, Fredrikson S, Masterman T, Jönsson B (2001) Costs, quality of life and disease severity in multiple sclerosis. A cross-sectional study in Sweden. Eur J Neurol 8: 27–35
Kobelt G, Lindgren P, Smala A, Jönsson B, Group GMS (2001) Costs and quality of life in multiple sclerosis. A cross-sectional observational study in Germany. Eur J Health Econ 2: 60–68
Acknowledgement
Ulrika Lilja (Stockholm Health Economics), Steve Hass (Elan Corporation)
Conflict of interest
No information supplied.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kobelt, G., Berg, J., Lindgren , P. et al. Costs and quality of life of multiple sclerosis in Austria. Eur J Health Econ 7 (Suppl 2), 14–23 (2006). https://doi.org/10.1007/s10198-006-0382-x
Issue Date:
DOI: https://doi.org/10.1007/s10198-006-0382-x