
Abstract
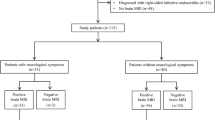
In infective endocarditis (IE), brain magnetic resonance imaging (MRI) is helpful to diagnose clinically silent neurological events. We assessed the usefulness of systematic early brain MRI in IE diagnosis and medico-surgical management. Over a period of 1 year, all patients admitted in one of the three hospitals participating in and fulfilling the Duke criteria for definite or possible IE underwent cerebral MRI within 7 days of IE suspicion. Eight panels of experts analyzed the records a posteriori. For each case, one record with and one record without the MRI results were randomly assigned to two panels, which determined the theoretical diagnosis and treatment. Paired comparisons were performed using a symmetry test. Thirty-seven brain MRIs were performed within a median of 5 days after inclusion. MRI was pathological in 26 patients (70 %), showing 62 % microischemia and 58 % microbleeds. The expert advice did not differ significantly between the two evaluations (with or without the MRI results). The therapeutic strategies determined diverged in five cases (13.5 %). Diagnosis differed in two cases (5.4 %), with an upgrading of diagnosis from possible to definite IE using MRI results. Early brain MRI did not significantly affect the IE diagnosis and medico-surgical treatment plan. These results suggest that systematic use of early brain MRI is irrelevant in IE. Further studies are necessary to define whether MRI is mandatory in IE management within a multidisciplinary approach, with particular attention paid to better timing and the subset of patients in whom this imaging examination could be beneficial.
Similar content being viewed by others

References
Sonneville R, Mourvillier B, Bouadma L, Wolff M (2011) Management of neurological complications of infective endocarditis in ICU patients. Ann Intensive Care 1:10
Sonneville R, Mirabel M, Hajage D et al (2011) Neurologic complications and outcomes of infective endocarditis in critically ill patients: the ENDOcardite en REAnimation prospective multicenter study. Crit Care Med 39:1474–1481
Corral I, Martín-Dávila P, Fortún J et al (2007) Trends in neurological complications of endocarditis. J Neurol 254:1253–1259
García-Cabrera E, Fernández-Hidalgo N, Almirante B et al (2013) Neurological complications of infective endocarditis: risk factors, outcome, and impact of cardiac surgery: a multicenter observational study. Circulation 127:2272–2284
Hoen B, Duval X (2013) Infective endocarditis. N Engl J Med 369:785
Corr P, Wright M, Handler LC (1995) Endocarditis-related cerebral aneurysms: radiologic changes with treatment. AJNR Am J Neuroradiol 16:745–748
Klein I, Iung B, Labreuche J et al (2009) Cerebral microbleeds are frequent in infective endocarditis: a case–control study. Stroke 40:3461–3465
Klein I, Iung B, Wolff M et al (2007) Silent T2* cerebral microbleeds: a potential new imaging clue in infective endocarditis. Neurology 68:2043
Duval X, Iung B, Klein I et al (2010) Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med 152:497–504, W175
Cooper HA, Thompson EC, Laureno R et al (2009) Subclinical brain embolization in left-sided infective endocarditis: results from the evaluation by MRI of the brains of patients with left-sided intracardiac solid masses (EMBOLISM) pilot study. Circulation 120:585–591
Thuny F, Avierinos J-F, Tribouilloy C et al (2007) Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur Heart J 28:1155–1161
Iung B, Klein I, Mourvillier B et al (2012) Respective effects of early cerebral and abdominal magnetic resonance imaging on clinical decisions in infective endocarditis. Eur Heart J Cardiovasc Imaging 13:703–710
Morofuji Y, Morikawa M, Yohei T et al (2010) Significance of the T2*-weighted gradient echo brain imaging in patients with infective endocarditis. Clin Neurol Neurosurg 112:436–440
Derex L, Bonnefoy E, Delahaye F (2010) Impact of stroke on therapeutic decision making in infective endocarditis. J Neurol 257:315–321
Habib G (2006) Management of infective endocarditis. Heart 92:124–130
Snygg-Martin U, Gustafsson L, Rosengren L et al (2008) Cerebrovascular complications in patients with left-sided infective endocarditis are common: a prospective study using magnetic resonance imaging and neurochemical brain damage markers. Clin Infect Dis 47:23–30
Champey J, Pavese P, Bouvaist H et al (2016) Cerebral imaging in infectious endocarditis: a clinical study. Infect Dis (Lond) 48:235–240. doi:10.3109/23744235.2015.1109704
Champey J, Pavese P, Bouvaist H, Kastler A, Krainik A, Francois P (2016) Value of brain MRI in infective endocarditis: a narrative literature review. Eur J Clin Microbiol Infect Dis 35:159–168. doi:10.1007/s10096-015-2523-6
Hess A, Klein I, Iung B et al (2013) Brain MRI findings in neurologically asymptomatic patients with infective endocarditis. AJNR Am J Neuroradiol 34:1579–1584
Goulenok T, Klein I, Mazighi M et al (2013) Infective endocarditis with symptomatic cerebral complications: contribution of cerebral magnetic resonance imaging. Cerebrovasc Dis 35:327–336
Barsic B, Dickerman S, Krajinovic V et al (2013) Influence of the timing of cardiac surgery on the outcome of patients with infective endocarditis and stroke. Clin Infect Dis 56:209–217
Habib G, Lancellotti P, Antunes MJ et al (2015) 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 36:3075–3128
Vilacosta I, Graupner C, San Román JA et al (2002) Risk of embolization after institution of antibiotic therapy for infective endocarditis. J Am Coll Cardiol 39:1489–1495
Kang D-H, Kim Y-J, Kim S-H et al (2012) Early surgery versus conventional treatment for infective endocarditis. N Engl J Med 366:2466–2473
Funakoshi S, Kaji S, Yamamuro A et al (2011) Impact of early surgery in the active phase on long-term outcomes in left-sided native valve infective endocarditis. J Thorac Cardiovasc Surg 142:836–842.e1
Piper C, Wiemer M, Schulte HD, Horstkotte D (2001) Stroke is not a contraindication for urgent valve replacement in acute infective endocarditis. J Heart Valve Dis 10:703–711
Ruttmann E, Willeit J, Ulmer H et al (2006) Neurological outcome of septic cardioembolic stroke after infective endocarditis. Stroke 37:2094–2099
Kim SJ, Lee JY, Kim TH et al (1998) Imaging of the neurological complications of infective endocarditis. Neuroradiology 40:109–113
Maxwell AE (1970) Comparing the classification of subjects by two independent judges. Br J Psychiatry 116:651–655
Botelho-Nevers E, Thuny F, Casalta JP et al (2009) Dramatic reduction in infective endocarditis-related mortality with a management-based approach. Arch Intern Med 169:1290–1298
Thuny F, Gaubert J-Y, Jacquier A et al (2013) Imaging investigations in infective endocarditis: current approach and perspectives. Arch Cardiovasc Dis 106:52–62
Loitfelder M, Seiler S, Schwingenschuh P, Schmidt R (2012) Cerebral microbleeds: a review. Panminerva Med 54:149–160
Greenberg SM, Vernooij MW, Cordonnier C et al (2009) Cerebral microbleeds: a guide to detection and interpretation. Lancet Neurol 8:165–174
Subramaniam S, Puetz V, Dzialowski I, Barber PA (2006) Cerebral microhemorrhages in a patient with mycotic aneurysm: relevance of T2-GRE imaging in SBE. Neurology 67:1697
Acknowledgments
We are grateful to the investigator groups: Prof. Carole Schwebel, Dr. Agnès Bonadona, Dr. Rebecca Hamiflar, Prof. Gerald Vanzetto, Dr. Géraldine Dessertaine, Dr. Aude Boignard, Dr. Caroline Augier, Dr. Isabelle Pierre, Dr. Jean-Paul Brion, and Dr. Claire Wintenberger for their respective participation in the expertise, and to Dr. Virginie Hincky-Vitrat and Dr. Emmanuel Forestier for their contribution to the inclusions.
We thank Raouf Zouglech, the clinical research assistant for this study.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Funding
None.
Conflict of interest
All authors: no conflicts.
Ethical approval
Yes.
Informed consent
Yes.
Additional information
Members of the investigator groups are listed at the end of the manuscript.
Rights and permissions
About this article

Cite this article
Champey, J., Pavese, P., Bouvaist, H. et al. Is brain angio-MRI useful in infective endocarditis management?. Eur J Clin Microbiol Infect Dis 35, 2053–2058 (2016). https://doi.org/10.1007/s10096-016-2764-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-016-2764-z