
ABSTRACT
Background
With the refinement of the technique, endoscopic endonasal surgery increases its field of indications. The orbital compartment is among the locations easily reached through the nostril. This anteromedial approach has been described primarily for inflammatory or traumatic diseases, with few data for tumoral diseases.
Method
Since 2010, this route has been used at our institution either for decompression or for biopsy of orbital tumoral diseases.
Findings/Conclusions
Even if further studies are warranted, this strategy proved to be beneficial for patients, with improvements in visual outcome. In this article, the authors summarize their technique and their experience with endonasal endoscopic orbital decompression.
Key points
• Nasal and sphenoidal anatomies determine the feasibility and risks for doing an efficient medial optic or orbit decompression.
• Techniques and tools used are those developed for pituitary surgery.
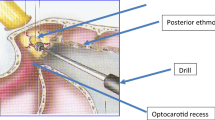
• A middle turbinectomy and posterior ethmoidectomy are mandatory to expose the medial wall of the orbit.
• The Onodi cell is a key marker for the optic canal and must be opened up with caution.
• The lamina papyracea is opened first with a spatula and the optic canal opened up by a gentle drilling under continuous irrigation from distal to proximal.
• Drilling might always be used under continuous irrigation to avoid overheating of the optic nerve. An ultrasonic device can be used as well.
• The nasal corridor is narrow and instruments may hide the infrared neuronavigation probe. To overcome this issue, a magnetic device could be useful.
• Doppler control could be useful to locate the ICA.
• The optic canal must be opened up from the tuberculum of the sella to the orbital apex and from the planum (anterior cranial fossa) to the lateral OCR or ICA canal
• At the end of the procedure, the optic nerve becomes frequently pulsatile, which is a good marker of decompression.





Similar content being viewed by others


References
Berhouma M, Messerer M, Jouanneau E (2012) Shifting paradigm in skull base surgery: Roots, current state of the art and future trends of endonasal endoscopic approaches. Rev Neurol (Paris) 168(2):121–134
Berhouma M, Messerer M, Jouanneau E (2012) Occam’s razor in minimally invasive pituitary surgery: tailoring the endoscopic endonasal uninostril trans-sphenoidal approach to sella turcica. Acta Neurochir (Wien). doi:10.1007/s00701-012-1510-2
Cebula H, Lahlou A, De Battista JC, Debry C, Froelich S (2010) Endoscopic approaches to the orbit. Neurochirurgie 56(2–3):230–235
Hart CK, Theodosopoulos PV, Zimmer LA (2009) Anatomy of the optic canal: a computed tomography study of endoscopic nerve decompression. Ann Otol Rhinol Laryngol 118(12):839–844
Jiang RS, Hsu CY, Shen BH (2001) Endoscopic optic nerve decompression for the treatment of traumatic optic neuropathy. Rhinology 39(2):71–74
Locatelli M, Caroli M, Pluderi M, Motta F, Gaini SM, Tschabitscher M, Scarone P (2011) Endoscopic transsphenoidal optic nerve decompression: an anatomical study. Surg Radiol Anat 33(3):257–262
Mariniello G, Bonavolontà G, Tranfa F, Maiuri F (2013) Management of the optic canal invasion and visual outcome in spheno-orbital meningiomas. Clin Neurol Neurosurg 115(9):1615–1620
Michel O, Oberländer N, Neugebauer P, Neugebauer A, Rüssmann W (2001) Follow-up of transnasal orbital decompression in severe Graves’ ophthalmopathy. Ophthalmology 108(2):400–404
Netuka D, Masopust V, Belšán T, Profantová N, Beneš V (2013) Endoscopic endonasal resection of medial orbital lesions with intraoperative MRI. Acta Neurochir (Wien) 155(3):455–461
Sia DIT, Chan WO, Wormald PJ, Davis G, Selva D (2012) Decompression of benign orbital apex lesion via medial endoscopic approach. Orbit 31(5):344–346
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
(MP4 240623 kb)
Rights and permissions
About this article

Cite this article
Jacquesson, T., Abouaf, L., Berhouma, M. et al. How I do it: the endoscopic endonasal optic nerve and orbital apex decompression. Acta Neurochir 156, 1891–1896 (2014). https://doi.org/10.1007/s00701-014-2199-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-014-2199-1