
Abstract
Objective
Decompressive craniectomy (DC) is efficient in reducing the intracranial pressure in several complicated disorders such as traumatic brain injury (TBI) and stroke. The neurosurgical procedure has indeed reduced the number of deaths. However, parallel with the reduced fatal cases, the number of vegetative patients has increased significantly. Mechanical stretching in axonal fibers has been suggested to contribute to the unfavorable outcome. Thus, there is a need for improving treatment procedures that allow both reduced fatal and vegetative outcomes. The hypothesis is that by performing the DC at the non-injured side of the head, stretching of axonal fibers at the injured brain tissue can be reduced, thereby having the potential to improve patient outcome.
Methods
Six patients, one with TBI and five with stroke, were treated with DC and where each patient’s pre- and postoperative computerized tomography (CT) were analyzed and transferred to a finite element (FE) model of the human head and brain to simulate DC both at the injured and non-injured sides of the head. Poroelastic material was used to simulate brain tissue.
Results
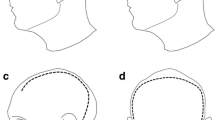
The computational simulation showed slightly to substantially increased axonal strain levels over 40 % on the injured side where the actual DC had been performed in the six patients. However, when the simulation DC was performed on the opposite, non-injured side, there was a substantial reduction in axonal strain levels at the injured side of brain tissue. Also, at the opposite, non-injured side, the axonal strain level was substantially lower in the brain tissue. The reduced axonal strain level could be verified by analyzing a number of coronal sections in each patient. Further analysis of axial slices showed that falx may tentatively explain part of the different axonal strain levels between the DC performances at injured and opposite, non-injured sides of the head.
Conclusions
By using a FE method it is possible to optimize the DC procedure to a non-injured area of the head thereby having the potential to reduce axonal stretching at the injured brain tissue. The postoperative DC stretching of axonal fibers may be influenced by different anatomical structures including falx. It is suggested that including computational FE simulation images may offer guidance to reduce axonal strain level tailoring the anatomical location of DC performance in each patient.





Similar content being viewed by others


References
Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM (2006) Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg 104:469–479
Bain AC, Meaney DF (2000) Tissue-level thresholds for axonal damage in an experimental model of central nervous system white matter injury. J Biomech Eng 122:615–622
Belytschko T, Liu W, Moran B, Elkhodary K (2013) Nonlinear finite elements for continua and structures. Wiley, New York
Bohman L, Schuster JM (2013) Decompressive craniectomy for management of traumatic brain injury: an update. Curr Neurol Neurosci Rep 13:1–8
Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D’Urso P, Kossmann T, Ponsford J, Seppelt I, Reilly P, Wolfe R; DECRA Trial Investigators; Australian and New Zealand Intensive Care Society Clinical Trials Group (2011) Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med 364(16):1493–1502
DeLorenzo C, Papademetris X, Staib LH, Vives KP, Spencer DD, Duncan JS (2012) Volumetric intraoperative brain deformation compensation: model development and phantom validation. IEEE Trans Med Imaging 31:1607–1619
Dumpuri P, Thompson RC, Dawant BM, Cao A, Miga MI (2007) An atlas-based method to compensate for brain shift: preliminary results. Med Image Anal 11:128–145
Dumpuri P, Thompson RC, Cao A, Ding S, Garg I, Dawant BM, Miga MI (2010) A fast and efficient method to compensate for brain shift for tumor resection therapies measured between preoperative and postoperative tomograms. IEEE Trans Biomed Eng 57:1285–1296
Honeybul S (2010) Complications of decompressive craniectomy for head injury. J Clin Neurosci 17:430–435
Honeybul S, Gillett G, Ho K, Lind C (2012) Ethical considerations for performing decompressive craniectomy as a life-saving intervention for severe traumatic brain injury. J Med Ethics 38:657–661. doi:10.1136/medethics-2012-100672
Hu J, Jin X, Lee JB, Zhang L, Chaudhary V, Guthikonda M, Yang KH, King AI (2007) Intraoperative brain shift prediction using a 3D inhomogeneous patient-specific finite element model. J Neurosurg 106:164–169
Kleiven S (2002) Finite element modeling of the human head. PhD Thesis, KTH, Stockholm
Li X, von Holst H, Kleiven S (2011) Influence of gravity for optimal head positions in the treatment of head injury patients. Acta Neurochir 153:2057–2064
Li X, von Holst H, Kleiven S (2013) Decompressive craniectomy causes a significant strain increase in axonal fiber tracts. J Clin Neurosci 20:509–513
Maréchal L (2009) Advances in octree-based all-hexahedral mesh generation: handling sharp features. In: Proceedings of the 18th International Meshing Roundtable, pp 65–84
Miga M, Paulsen K, Kennedy F, Hartov A, Roberts D (1999) Model-updated image-guided neurosurgery using the finite element method: incorporation of the falx cerebri. In: MICCAI’99, Springer, Berlin Heidelberg New York, pp 900–909
Miga MI, Paulsen KD, Hoopes PJ, Kennedy FE Jr, Hartov A, Roberts DW (2000) In vivo quantification of a homogeneous brain deformation model for updating preoperative images during surgery. IEEE Trans Biomed Eng 47:266–273
Otsu N (1979) A threshold selection method from gray-level histogram. IEEE Trans Syst Man Cybern Syst 9:62–66
Pieper S, Halle M, Kikinis R (2004) 3D slicer. In: Proc IEEE Int Symp Biomed Imaging, IEEE, pp 632–635
Schneider GH, Bardt T, Lanksch WR, Unterberg A (2002) Decompressive craniectomy following traumatic brain injury: ICP, CPP and neurological outcome. Acta Neurochir Suppl 81:77–79
Stiver SI (2009) Complications of decompressive craniectomy for traumatic brain injury. Neurosurg Focus 26:7
von Holst H (2007) Traumatic brain injury. In: Feigin VL, Bennett DA (eds) Handbook of clinical neuroepidemiology. Nova Science, New York, pp 197–232
von Holst H, Li X (2013) Numerical impact simulation of gradually increased kinetic energy transfer has the potential to break up folded protein structures resulting in cytotoxic brain tissue edema. J Neurotrauma 30:1192–1199
von Holst H, Li X, Kleiven S (2012) Increased strain levels and water content in brain tissue after decompressive craniotomy. Acta Neurochir 154:1583–1593
Wittek A, Joldes G, Couton M, Warfield SK, Miller K (2010) Patient-specific non-linear finite element modelling for predicting soft organ deformation in real-time; application to non-rigid neuroimage registration. Prog Biophys Mol Biol 103:292–303
Yu Z, Morrison B (2010) Experimental mild traumatic brain injury induces functional alteration of the developing hippocampus. J Neurophysiol 103:499–501
Acknowledgments
The present study was supported by the research foundations at Karolinska University Hospital, Stockholm County, and division of Neuronic engineering at KTH, Sweden
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
The authors present an interesting study using the finite elements to determine the correlation between the strain level and axonal function in traumatic brain injury or stroke. From the computational simulation in the present study it was found that by performing decompressive craniectomy at the opposite, non-injured side, the axonal strain level decreased not only at the injured side but also on the opposite, non-injured side. This study represents a significant step in introducing the finite-elements thinking in the neurosurgical community. This method is of interest for the development of new innovative ways in neurosurgery.
A. Alfieri,
Neuruppin, Germany
Rights and permissions
About this article

Cite this article
von Holst, H., Li, X. Decompressive craniectomy (DC) at the non-injured side of the brain has the potential to improve patient outcome as measured with computational simulation. Acta Neurochir 156, 1961–1967 (2014). https://doi.org/10.1007/s00701-014-2195-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-014-2195-5