
Abstract
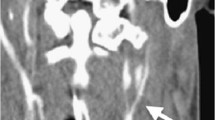
Almost all cases of carotid artery injury are precipitated by a high-energy impact such as motor vehicle accidents or gunshot wounds, and are usually diagnosed using angiography. We report herein a case of carotid artery injury induced by a low-energy insult with rare clinical signs which was diagnosed using ultrasonography as well as angiography. A 37-year-old man sustained an accidental compression of the neck and was transferred to our emergency room. Horner’s syndrome and phrenic nerve palsy were detected on the left side. Ultrasonography demonstrated two sites of injury with an intimal flap of the distal left common carotid artery as well as angiography. The patient was placed on anticoagulants and was discharged on the 10th hospital day with both Horner’s syndrome and phrenic nerve palsy. This case suggests that surgeons should investigate any possible carotid artery injury, even after low-velocity injuries such as compression of the neck, and therefore an ultrasonic examination should be performed at the initial evaluation and at follow-up studies. In addition, further investigations are also called for to investigate the utility of anticoagulation in the treatment of carotid artery injury.
Similar content being viewed by others


References
Davis JW, Holbrook TL, Hoyt DB, Mackersie RC, Field TO, Shackford SR (1990) Blunt carotid artery dissection: incidence, associated injuries, screening, and treatment. J Trauma 30:1514–1517
Fabian TC, Patton JH, Croce MA, Minard G, Kudsk KA, Pritchard E (1996) Blunt carotid injury. Importance of early diagnosis and anticoagulant therapy. Ann Surg 223:513–525
Li MS, Smith BM, Espinosa J, Brown RA, Richardson P, Ford R (1994) Nonpenetrating trauma to the carotid artery: seven cases and a literature review. J Trauma 36:265–272
Pretre R, Reverdin A, Kalonji T, Faidutti B (1994) Blunt carotid artery injury: difficult therapeutic approaches for an underrecognized entity. Surgery 115:375–381
Cooper A, Barlow B, Niemirska M, Gandhi R (1987) Fifteen years’ experience with penetrating trauma to the head and neck in children. J Pediatr Surg 22:24–27
Hall JR, Reyes HN, Meller JL (1991) Penetrating zone II neck injuries in children. J Trauma 31:1614–1617
Robbs JV, Human RR, Rajaruthnam P, Duncan H, Vawda I, Baker LW (1983) Neurological deficit and injuries involving the neck arteries. Br J Surg 70:220–222
Eachempati SR, Vaslef SN, Sebastian MW, Reed RL II (1998) Blunt vascular injuries of the head and neck: is heparinization necessary? J Trauma 45:997–1004
Yang X, Virtaniemi J, Vuorenniemi R (1995) Asymptomatic carotid artery occlusion from a gunshot. The role of angiography in penetrating neck trauma. Eur Arch Otorhinolaryngol 252:440–442
Perry MO, Snyder WH, Thal ER (1980) Carotid artery injuries caused by blunt trauma. Ann Surg 192:74–77
Colella JJ, Diamond DL (1996) Blunt carotid injury: reassessing the role of anticoagulation. Am Surg 3:212–217
Stain SC, Yellin AE, Weaver FA, Pentecost MJ (1989) Selective management of nonocclusive arterial injuries. Arch Surg 124: 1136–1141
Mokri B (1990) Traumatic and spontaneous extracranial internal carotid artery dissections. J Neurol 237:356–361
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Matsumoto, H., Noji, Y., Hirota, K. et al. Blunt carotid artery injury after accidental neck compression: Report of a case. Surg Today 30, 477–480 (2000). https://doi.org/10.1007/s005950050630
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s005950050630