
Abstract
Purpose
Indicating lumbar disc herniation via magnetic resonance imaging (MRI) T2 mapping in the posterior annulus fibrosus (AF).
Methods
Sagittal T2 maps of 313 lumbar discs of 64 patients with low back pain were acquired at 3.0 Tesla (3T). The discs were rated according to disc herniation and bulging. Region of interest (ROI) analysis was performed on median, sagittal T2 maps. T2 values of the AF, in the most posterior 10% (PAF-10) and 20% of the disc (PAF-20), were compared.
Results
A significant increase in the T2 values of discs with herniations affecting the imaged area, compared to bulging discs and discs with lateral herniation, was shown in the PAF-10, where no association to the NP was apparent. The PAF-20 exhibited a moderate correlation to the nucleus pulposus (NP).
Conclusions
High T2 values in the PAF-10 suggest the presence of disc herniation (DH). The results indicate that T2 values in the PAF-20 correspond more to changes in the NP.
Similar content being viewed by others
Introduction
Intervertebral disc degeneration and disc herniation are considered to be the main causes of low back pain, although the exact mechanisms of pain generation are not fully elucidated [1, 2]. Factors contributing to the development of back pain, disc degeneration, and disc herniation are manifold [2–6]. Back pain seems to be more prevalent in the lower than in the upper lumbar spine [7]. Apart from morphological changes, pathological discs can be distinguished by their water content and distribution of collagen. Normal discs are characterized by higher water content in the nucleus pulposus (NP) than in the annulus fibrosus (AF) [8, 9]. Magnetic resonance imaging (MRI) is a well-established, non-invasive method for the assessment of intervertebral discs and their pathologies [10].
T2 mapping visualizes variations in collagen orientation and water mobility. The changes in the biochemical composition during disc degeneration promote a change in T2 relaxation times [11]. T2 maps therefore allow for a quantitative approach to the question of whether different types of disc pathologies can be differentiated via MRI [12–15]. It is important to notice that T2 values are also dependent on other factors, such as age [16].
It is generally accepted that the posterior AF is a crucial structure in the development of posterior intervertebral disc herniation (DH) [17]. In normal discs, fibrocartilage like the posterior AF exhibits a dense collagen network and low water content, indicated by low T2 values [11]. The stiffness and strength of the tissue increase from the inner AF to the outer AF [18]. High T2 values in the posterior AF may indicate a structural weakness of the collagen structure and/or higher water content. The literature suggests that the T2 relaxation time of the posterior AF could be useful for the evaluation of present or imminent DH [13, 19].
Recommendations by the North American Spine Society, the American Society of Spine Radiology, and the American Society of Neuroradiology authored by Fardon and Milette in 2001 classify degenerative lumbar disc disease as follows. In a herniated disc, the herniation may take up to 50% of the circumference of the disc. In this case, the AF is not intact. Herniated discs can be further subdivided into protruded and extruded discs. A general disc displacement taking up more than 50% of the circumference is termed bulging. It usually does not extend far from the apophysis [20]. The Pfirrmann score is used to grade discs on sagittal images on a scale from one to five based on sagittal T2-weighted images [21]. In a study concerning sodium MRI and T2 mapping, a significant negative correlation between the modified Pfirrmann score [22] and T2 mapping has been demonstrated [23]. Another work comes to the conclusion that T2 mapping is more suitable for the assessment of early cervical disc degeneration, after finding that NP T2 values show a strong and negative correlation with the Pfirrmann score, but AF T2 values do not [24]. Another study found the Pfirrmann score to be dependent on age and anatomical disc level [25]. The progression of discs in MRI could give an indication to predict future DH. A possible location for this would be the AF, as its structural weakening is thought to play a role in DH. However, it is not known which part of the posterior AF should be evaluated to predict the presence of DH. The aim of this study was to compare two evaluation approaches for the posterior AF with regard to indication of the presence of DH.
Materials and methods
Study design and study subjects
Ethical permission was granted by the local ethics commission. Oral and written informed consent was obtained from all study participants. The study was performed as a cross-sectional study in patients with low back pain. Patients with single or recurrent episodes of low back pain, above 18 years of age and below 65 years of age, and who were actively working, were included. Exclusion criteria were radicular pain, neurological deficits of the lower limb, known lumbar disc herniation within the last 2 years, previous spine surgery, lumbosacral transitional vertebrae, and contraindications for MRI.
Twenty-one male and 43 female individuals were included in this study, for a total of 64 subjects. The mean age was 38.5 ± 10.7 years (range 18–64), with 36.2 ± 9.5 years (range 23–52) for men and 39.6 ± 11.2 years (range 18–64) for women.
Magnetic resonance imaging
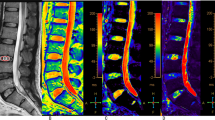
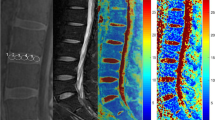
MR examinations were performed on a 3.0 Tesla (3T) whole-body scanner (Tim Trio, Siemens Medical Solutions, Erlangen, Germany) using a dedicated eight-channel spine coil (3T Spine Matrix Coil, Siemens). Subjects were scanned in the supine position. T1- and T2-weighted fast spin echo (FSE) sequences in the sagittal and axial plane were used for morphological evaluation. For T2 mapping, a multi-echo spin echo sequence was used (repetition time (TR) = 1200 ms; echo time (TE) = 13.8 ms, 27.6 ms, 41.4 ms, 55.2 ms, 69.0 ms, 82.8 ms; field of view (FOV): 220 × 220 mm2; pixel matrix: 256 × 256; voxel size: 0.86 × 0.86 × 5 mm3; number of sagittal slices: 10; interslice gap: 1 mm; examination time: 7:45 min). T2 maps were obtained using a pixel-wise, mono-exponential non-negative least squares (NNLS) fit analysis (MapIt, Siemens Medical Solutions, Erlangen, Germany) (Fig. 1).

Example of sagittal lumbar disc T2 mapping (L3–S1) laid over a T2 FSE spine image. The Pfirrmann score for these discs was 2 for the L3/L4 and L5/S1 discs and 3 for the L4/L5 disc; the L4/L5 disc is herniated, and the L3/L4 and L5/S1 discs show bulging. Higher T2 levels in the most posterior part of the posterior AF of the herniated disc are noticeable. Image reproduced from: Trattnig et al. [13]
Image analysis
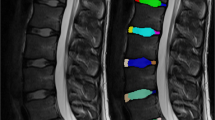
T1- and T2-weighted FSE sequences in the sagittal and axial plane were used for morphological evaluation. All discs were rated by an experienced, senior musculoskeletal radiologist using the guidelines for the classification of disc pathology by Fardon and Milette. Adhering to this, discs with “localized displacement of” disc material “beyond the intervertebral disc space” taking up under 180° of the disc circumference were labeled herniation. Disc material displacement over 180° of the circumference was counted as bulging discs [20]. The Pfirrmann score was used to evaluate disc degeneration [21]. The T2 relaxation times of the AF were assessed on the T2 maps by means of region-of-interest (ROI) analysis. All evaluations were performed on the two most central sagittal slices. More lateral sagittal slices were not included in the evaluation to avoid partial volume effects. Two approaches were chosen to evaluate the posterior AF: a rectangular ROI covering (1) the posterior 20% of the mid-sagittal disc diameter (PAF-20); and (2) the posterior 10% of the mid-sagittal disc diameter (PAF-10) (Fig. 2). To this end, the disc was divided into five equal parts with rectangular ROIs of the same dimensions. For (1), the most posterior ROI (=PAF-20) was chosen. For (2), another ROI was drawn in the PAF-20, covering exactly the posterior half of it (=PAF-10). The NP was evaluated by a rectangular ROI that included the middle 60% of the disc. Discs with high-intensity zones (HIZ) were excluded (N = 2 discs), since this would bias T2 measurements in the posterior AF. Tears of the AF, observed as an HIZ, have already been found to not influence future disc degeneration [26]. The discs were then grouped according to whether they presented with displaced disc material and whether there was a herniation affecting the disc area that was imaged. Group one (G1) comprises normal discs. Group two (G2) includes lateral DH (five discs) and bulging discs, graded using the system by Fardon and Milette [20]. This group aims to gather all disc material displacements, where no herniation is directly visible on the two chosen slices, and thus no annular rupture. Group three (G3) comprises discs with focal posterior DH in the median, mediolateral, or paramedian position, again graded by Fardon and Milette [20]. In these cases, it was certain that the selected imaging slices would be affected (central 11 mm = central two sagittal slices). This grouping does not aim to be its own grading system, but gathers discs that the authors believe might share similarities in the most posterior part of the AF with regard to the MRI slices used. If artifacts reached into the region of interest, single discs were excluded (N = 5 discs). All in all, 313 lumbar discs were evaluated.

Model of ROI placement. The posterior AF was assessed using two different approaches: The most posterior 10% and 20% of the disc in a sagittal T2 map slice
Statistical analysis
The statistical evaluation was performed using PASW Statistics 19.0 (SPSS, IBM, Chicago, IL, USA). The mean T2 values of the different regions were compared using a one-way analysis of variance (ANOVA) with Tukey post hoc tests. A Pearson correlation was used to measure the association between PAF-20 and NP and between PAF-10 and NP. The strength of association was determined by considering the correlation coefficients and their significance. A correlation was considered very strong if there was an absolute value of 0.80–1.00, a strong correlation by 0.60–0.79, a moderate correlation by 0.40–0.59, a weak correlation by 0.20–0.39, and no correlation by an absolute value under 0.20. A stepwise logistic regression was performed for the binary outcome variable “G3” and covariates PAF-20 and PAF-10 (step size 10 ms).
Results
Morphological MRI findings
One hundred and thirty-six discs (43.5%) were healthy and showed no herniation or bulging. One hundred and thirty-five discs (43.1%) were graded as bulging and 42 discs (13.4%) as herniated. Twenty-four instances of DH (57.1%) were found in the median disc section, 11 (26.2%) in the mediolateral area, 2 (4.8%) in the paramedian region, and 5 (11.9%) in the lateral area. This resulted in the following groups: G1 including all healthy discs, G2 comprising all bulging discs, and lateral DH (N = 140; 44.7%) and G3 containing median, mediolateral, and perimedian DH (N = 37; 11.82%) (Fig. 3).

Number of discs in the groups according to location
Using the Pfirrmann score, two discs were classified as grade 1 (0.6%), 182 discs as grade 2 (58.1%), 92 discs as grade 3 (29.4%), 36 discs as grade 4 (11.5%), and 1 disc as grade 5 (0.3%) (Fig. 4). In G1 discs, the mean Pfirrmann score was 2.28 (sd = 0.58), in G2 discs 2.61 (sd = 0.717), and in G3 discs 3.14 (sd = 0.751).

Mean T2 relaxation times of the annulus fibrosus measured in the most posterior 10% and 20% of the disc. In contrast to the PAF-20, the PAF-10 showed elevated T2 values in G3. See also Table 1
T2 mapping results
The mean T2 relaxation time for the PAF-10 and the PAF-20 in all groups can be found in Table 1 and Fig. 4. The T2 values were found to be significantly higher in the PAF-10 of G3 discs than in those of G2 discs (p = 0.042). The comparison of PAF-10 between G1 and G3 discs showed a tendency for higher T2 values in the G3 discs (p = 0.062) as well. However, the T2 values of the PAF-10 were very similar in G1 and G2 discs (p = 0.970). For the PAF-10 and the NP, there was no association, with a Pearson correlation coefficient of 0.050 (p = 0.380). The logistic regression showed an estimated odds ratio for G3 of 2.57 for a 10 ms increase in T2 values in the PAF-10.
In the PAF-20, the G1 discs showed significantly higher T2 relaxation times than both G2 discs and G3 discs (both p < 0.001). Although the G2 discs showed higher T2 values than the G3 discs, this difference was non-significant (p = 0.159). The Pearson correlation between the PAF-20 and the NP was significant (p < 0.001), with a Pearson coefficient of 0.448. The logistic regression showed an estimated odds ratio of 0.51 for a 10 ms increase in T2 values in the PAF-20.
This study aimed to provide insight into the question of whether T2 mapping could aid in the prediction of disc herniation. T2 values were analyzed in the most posterior parts of the AF, to demonstrate differences between herniated, bulging, and normal discs. The comparison of T2 values resulted in different findings for the PAF-10 and the PAF-20. Overall, the PAF-20 showed mean T2 relaxation times of about 27.4 ms higher than those of the PAF-10. In the PAF-20, both G2 and G3 discs showed significantly lower T2 values than normal discs (both p < 0.001). There was no significant difference between the PAF-20 T2 values of G2 and G3 discs (p = 0.195). In a previous study, T2 relaxation times of the posterior 20% of the disc were found to be significantly lower in discs with bulging or herniation compared to normal discs as well [13]. In the PAF-10, the mean T2 value of G3 discs was about 3.5 ms greater than in the G2 discs. This difference was, however, only at the border of significance (p = 0.042). Concluding, G3 discs differed significantly from G2 discs in the PAF-10 and from G1 discs in the PAF-20. The results indicate that a certain pattern of T2 relaxation times in the PAF-10 and the PAF-20 may be characteristic for disc herniation. It appears that even small structural changes in the posterior parts of the posterior annulus, indicated by an increase of T2 relaxation times, are associated with the presence of disc herniation. The Pearson correlation suggests that while the PAF-20 T2 values are connected to those of the NP, the PAF-10 is an independent variable. As such, the PAF-10 might be able to represent solely the status of the posterior AF, without taking into account changes in the NP. A comparison of the values found in the NP, PAF-20, and PAF-10 is given in Fig. 5. Thus, we favor the PAF-10 region as the critical region for the assessment of structural weakness of the AF and the prediction of DH.

T2 relaxation times of the NP, PAF-20, and PAF-10. In comparison to the PAF-10, the PAF-20 shows values closer to the NP
Discussion
Logistic regression indicates that a higher PAF-10 T2 value raises the odds that a disc is herniated. The presence of DH in discs with increased T2 values in the posterior part of the posterior AF (PAF-10 in our study) is not surprising. T2 relaxation times in the AF are usually low and a change thereof may indicate structural degradation. For the first time, this study quantifies the association between T2 values in different regions of the AF and the presence of DH. This cross-sectional data help to design future longitudinal studies to assess the value of T2 values for future DH.
Interestingly, higher T2 values in the PAF-20 decreased the odds of disc herniation in our study. Another study found lower T2 values in the posterior AF in herniated discs in comparison to normal discs [13]. Similarly, Ogon et al., using a similar ROI analysis by dividing the disc into five parts, observed lower T2 relaxation times of the posterior AF in patients with chronic lower back pain [19]. This could be explained by the observation that the anterior part of the posterior AF is heavily influenced by the state of the NP. If the water content in the nucleus is high, it is likely that the anterior part of the posterior AF also has higher water content. This might be even more likely when the anterior part of the posterior AF shows signs of early degeneration, with the posterior part of the posterior AF being the last barrier preventing disc material from herniating. Trattnig et al. found that NP of discs with herniations or annular tears had lower T2 values on average [13].
A disc with a great likelihood of herniation would, therefore, show high T2 relaxation times in the PAF-10, but low T2 relaxation times in the PAF-20.
A paper by Stelzeneder et al. shows low T2 values in the AF of Pfirrmann Grade I discs and high T2 values in Grade II, declining through Grade III and IV [27]. While our results reflect this behavior for the PAF-20, in the PAF-10 T2 values rise until Grade III and decline thereafter.
The limitations of this study include the cross-sectional design of our study. Thus, no predictions about future disc herniation risk are possible. Furthermore, clinical evaluation of patients using questionnaires was not available for our study. A further limitation might be the exclusion of discs with HIZ, as this presents the exclusion of a specific group of extruded discs. HIZ are defined as high T2 values and inclusion of these discs would certainly produce a great difference between disc herniation and all other discs. These high T2 values would, however, be a mixture of two very different groups. This means, of course, that there might be “HIZ” subresolution, changing the values in herniated discs that are not visible to the examiner.
The grading system used in this study has been shown to have relatively good inter-observer agreement [28]. As for the ROI analysis, the inter- and intra-observer agreement has been shown to be strong and medium to strong for the posterior AF [27, 29]. In the future, autosegmentation might provide an interesting alternative [30].
In conclusion, this in vivo study demonstrates that disc herniation is more likely to be present if the posterior part of the posterior AF shows structural weakening (indicated by increased T2 values). Our data suggest that the structural weakness of this part of the lumbar intervertebral disc can be measured quantitatively using T2 mapping in patients with low back pain.
Future longitudinal studies are needed to elucidate whether the rise in T2 values in the posterior part of the posterior AF precedes disc herniation. This could help to predict future disc herniation and to allow for tailored individual therapy programs, potentially preventing disc herniation in patients with low back pain.
References
Carragee EJ (2005) Clinical practice. Persistent low back pain. N Engl J Med 352(18):1891–1898
Battie MC, Videman T (2006) Lumbar disc degeneration: epidemiology and genetics. J Bone Joint Surg Am 88(Suppl 2):3–9
Miller JA, Schmatz C, Schultz AB (1988) Lumbar disc degeneration: correlation with age, sex, and spine level in 600 autopsy specimens. Spine (Phila Pa 1976) 13(2):173–178
Evans W, Jobe W, Seibert C (1989) A cross-sectional prevalence study of lumbar disc degeneration in a working population. Spine (Phila Pa 1976) 14(1):60–64
Riihimaki H, Mattsson T, Zitting A, Wickstrom G, Hanninen K, Waris P (1990) Radiographically detectable degenerative changes of the lumbar spine among concrete reinforcement workers and house painters. Spine (Phila Pa 1976) 15(2):114–119
Videman T, Sarna S, Battie MC, Koskinen S, Gill K, Paananen H, Gibbons L (1995) The long-term effects of physical loading and exercise lifestyles on back-related symptoms, disability, and spinal pathology among men. Spine (Phila Pa 1976) 20(6):699–709
Videman T, Battie MC, Gill K, Manninen H, Gibbons LE, Fisher LD (1995) Magnetic resonance imaging findings and their relationships in the thoracic and lumbar spine. Insights into the etiopathogenesis of spinal degeneration. Spine (Phila Pa 1976) 20(8):928–935
Antoniou J, Steffen T, Nelson F, Winterbottom N, Hollander AP, Poole RA, Aebi M, Alini M (1996) The human lumbar intervertebral disc: evidence for changes in the biosynthesis and denaturation of the extracellular matrix with growth, maturation, ageing, and degeneration. J Clin Invest. 98(4):996–1003
Ludescher B, Effelsberg J, Martirosian P, Steidle G, Markert B, Claussen C, Schick F (2008) T2- and diffusion-maps reveal diurnal changes of intervertebral disc composition: an in vivo MRI study at 1.5 Tesla. J Magn Reson Imaging 28(1):252–257
Modic MT, Ross JS (2007) Lumbar degenerative disk disease. Radiology 245(1):43–61
Weidenbaum M, Foster RJ, Best BA, Saed-Nejad F, Nickoloff E, Newhouse J, Ratcliffe A, Mow VC (1992) Correlating magnetic resonance imaging with the biochemical content of the normal human intervertebral disc. J Orthop Res 10(4):552–561
Perry J, Haughton V, Anderson PA, Wu Y, Fine J, Mistretta C (2006) The value of T2 relaxation times to characterize lumbar intervertebral disks: preliminary results. AJNR Am J Neuroradiol 27(2):337–342
Trattnig S, Stelzeneder D, Goed S, Reissegger M, Mamisch TC, Paternostro-Sluga T, Weber M, Szomolanyi P, Welsch GH (2010) Lumbar intervertebral disc abnormalities: comparison of quantitative T2 mapping with conventional MR at 3.0 T. Eur Radiol 20(11):2715–2722
Tertti M, Paajanen H, Laato M, Aho H, Komu M, Kormano M (1991) Disc degeneration in magnetic resonance imaging. A comparative biochemical, histologic, and radiologic study in cadaver spines. Spine (Phila Pa 1976) 16(6):629–634
Watanabe A, Benneker LM, Boesch C, Watanabe T, Obata T, Anderson SE (2007) Classification of intervertebral disk degeneration with axial T2 mapping. AJR Am J Roentgenol 189(4):936–942
Wang YXJ, Griffith JF, Leung JCS, Yuan J (2014) Age related reduction of T1rho and T2 magnetic resonance relaxation times of lumbar intervertebral disc. Quant Imaging Med Surg 4(4):259–264
Coventry MB, Ghormley RK, Kernohan JW (1945) The intervertebral disc: its microscopic anatomy and pathology: II. Changes in the intervertebral disc concomitant with age. J Bone Joint Surg Am 27(2):233–247
Shan Z, Li S, Liu J, Mamuti M, Wang C, Zhao F (2015) Correlation between biomechanical properties of the annulus fibrosus and magnetic resonance imaging (MRI) findings. Eur Spine J 24(9):1909–1916
Ogon I, Takebayashi T, Takashima H, Tanimoto K, Ida K, Yoshimoto M, Fujiwara H, Kubo T, Yamashita T (2015) Analysis of chronic low back pain with magnetic resonance imaging T2 mapping of lumbar intervertebral disc. J Orthop Sci. 20(2):295–301
Fardon DF, Milette PC (2001) Nomenclature and classification of lumbar disc pathology. Recommendations of the Combined task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine (Phila Pa 1976) 26(5):E93–E113
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N (2001) Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 26(17):1873–1878
Griffith JF, Wang YX, Antonio GE, Choi KC, Yu A, Ahuja AT, Leung PC (2007) Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 32(24):E708–E712
Noebauer-Huhmann IM, Juras V, Pfirrmann CW, Szomolanyi P, Zbyn S, Messner A, Wimmer J, Weber M, Friedrich KM, Stelzeneder D, Trattnig S (2012) Sodium MR imaging of the lumbar intervertebral disk at 7 T: correlation with T2 mapping and modified Pfirrmann score at 3 T–preliminary results. Radiology 265(2):555–564
Chen C, Huang M, Han Z, Shao L, Xie Y, Wu J, Zhang Y, Xin H, Ren A, Guo Y, Wang D, He Q, Ruan D (2014) Quantitative T2 magnetic resonance imaging compared to morphological grading of the early cervical intervertebral disc degeneration: an evaluation approach in asymptomatic young adults. PLoS One 9(2):e87856
Ulbrich EJ, Anon J, Hodler J, Zimmermann H, Sturzenegger M, Anderson SE, Boesch C (2014) Does normalized signal intensity of cervical discs on T2 weighted MRI images change in whiplash patients? Injury. 45(4):784–791
Farshad-Amacker NA, Hughes AP, Aichmair A, Herzog RJ, Farshad M (2014) Is an annular tear a predictor for accelerated disc degeneration? Eur Spine J 23(9):1825–1829
Stelzeneder D, Welsch GH, Kovács BK, Goed S, Paternostro-Sluga T, Vlychou M, Friedrich K, Mamisch TC, Trattnig S (2011) Quantitative T2 evaluation at 3.0T compared to morphological grading of the lumbar intervertebral disc: A standardized evaluation approach in patients with low back pain. Eur J Radiol. doi:10.1016/j.ejrad.2010.12.093
Li Y, Frederickson V, Resnick DK (2015) How should we grade lumbar disc herniation and nerve root compression? A systematic review. Clin Orthop Relat Res 473:1896–1902
Nilsson M, Lagerstrand K, Kasperska I, Brisby H, Hebelka H (2016) Axial loading during MRI influences T2-mapping values of lumbar discs: a feasibility study on patients with low back pain. Eur Spine J. doi:10.1007/s00586-016-4670-6
Castro-Mateos I, Pozo JM, Eltes PE, Del Rio L, Lazary A, Frangi AF (2014) 3D segmentation of annulus fibrosus and nucleus pulposus from T2-weighted magnetic resonance images. Phys Med Biol 59(24):7847–7864
Acknowledgements
Open access funding provided by Medical University of Vienna. Funding for this study was provided by the Austrian Science Fund (FWF): TRP-L194-B05. The authors thank Claudia Kronnerwetter, Manuela Karner, and Christine Penz for their technical support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Messner, A., Stelzeneder, D., Trattnig, S. et al. Does T2 mapping of the posterior annulus fibrosus indicate the presence of lumbar intervertebral disc herniation? A 3.0 Tesla magnetic resonance study. Eur Spine J 26, 877–883 (2017). https://doi.org/10.1007/s00586-016-4873-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4873-x