
Abstract
Purpose
Tracheostomy may become indispensable for patients with acute traumatic cervical spinal cord injuries. However, the early prediction of a tracheostomy is often difficult. Previous prediction models using the pulmonary function test (PFT) have limitations because some severely injured patients could not provide acceptable PFT results. We aim to develop an alternative model for predicting tracheostomy using accessible data obtained from the bedside.
Method
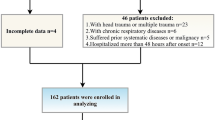
Clinical, neurological and radiological data from 345 consecutive patients with acute tetraplegia were retrospectively reviewed. We applied multiple logistic regression analysis (MLRA) and classification and regression tree (CART) analysis to develop the prediction model for tracheostomy. By train-test cross-validation, we used the sensitivity, specificity, area under the receiver operating characteristics curve (AUC) and correction rate to evaluate the performance of these models.
Results
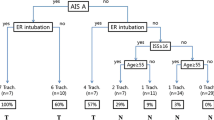
According to the American Spinal Injury Association (ASIA) standards, an admission ASIA motor score (AAMS) ≤ 22, ASIA grade A and presence of respiratory complications were identified as independent predictors of tracheostomy by both models. The model derived by CART suggested that the highest signal change (HSC) in the spinal cord on magnetic resonance imaging (MRI) also affected a patient’s requirement for a tracheostomy, while MLRA demonstrated that tracheostomy was also influenced by the presence of an ASIA grade B injury. The CART model had a sensitivity of 73.7 %, specificity of 89.7 %, AUC of 0.909 and overall correction rate of 87.3 %. The sensitivity, specificity, AUC and correction rate of the MLRA model were 81.8, 86.4, 0.889 and 85.7 %, respectively.
Conclusions
We suggest using the CART model in clinical applications. Patients with AAMS ≤ 1 exhibit an increased likelihood of requiring a tracheostomy. For patients with an AAMS in the range of 2–22, surgeons should consider giving these patients a tracheostomy once respiratory complications occur. Surgeons should be cautious to give a tracheostomy to patients with an AAMS ≥ 23, if the patient experiences an incomplete spinal cord injury and the HSC in the spinal cord is at C3 level or lower based on MRI. For other patients, close observation is necessary; generally, patients with complete SCI might require a tracheostomy more frequently.




Similar content being viewed by others

References
[No authors listed]. Spinal cord injury facts and figures at a glance. (2014) J Spinal Cord Med 37(4):479–480
Berney S, Bragge P, Granger C, Opdam H, Denehy L (2011) The acute respiratory management of cervical spinal cord injury in the first 6 weeks after injury: a systematic review. Spinal Cord 49(1):17–29
Romero J, Vari A, Gambarrutta C, Oliviero A (2009) Tracheostomy timing in traumatic spinal cord injury. Eur Spine J 18(10):1452–1457
Griffiths J, Barber VS, Morgan L, Young JD (2005) Systematic review and meta-analysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation. BMJ 330(7502):1243
Lissauer ME (2013) Benefit, timing and technique of tracheostomy. Curr Probl Surg 50(10):494–499
Durbin CG Jr (2010) Tracheostomy: why, when, and how? Respir Care 55(8):1056–1068
Berney SC, Gordon IR, Opdam HI, Denehy L (2011) A classification and regression tree to assist clinical decision making in airway management for patients with cervical spinal cord injury. Spinal Cord 49(2):244–250
Yugué I, Okada S, Ueta T et al (2012) Analysis of the risk factors for tracheostomy in traumatic cervical spinal cord injury. Spine (Phila Pa 1976) 37(26):E1633–E1638
Menaker J, Kufera JA, Glaser J, Stein DM, Scalea TM (2013) Admission ASIA motor score predicting the need for tracheostomy after cervical spinal cord injury. J Trauma Acute Care Surg 75(4):629–634
Harrop JS, Sharan AD, Scheid EH Jr, Vaccaro AR, Przybylski GJ (2004) Tracheostomy placement in patients with complete cervical spinal cord injuries: American Spinal Injury Association Grade A. J Neurosurg 100(1 Suppl Spine):20–23
Leelapattana P, Fleming JC, Gurr KR, Bailey SI, Parry N, Bailey CS (2012) Predicting the need for tracheostomy in patients with cervical spinal cord injury. J Trauma Acute Care Surg 73(4):880–884
Nakashima H, Yukawa Y, Imagama S et al (2013) Characterizing the need for tracheostomy placement and decannulation after cervical spinal cord injury. Eur Spine J 22(7):1526–1532
Maynard FM Jr, Bracken MB, Creasey G et al (1997) International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association. Spinal Cord 35(5):266–274
Fehlings MG, Rao SC, Tator CH et al (1999) The optimal radiologic method for assessing spinal canal compromise and cord compression in patients with cervical spinal cord injury. Part II: results of a multicenter study. Spine (Phila Pa 1976) 24(6):605–613
Furlan JC, Fehlings MG, Massicotte EM et al (2007) A quantitative and reproducible method to assess cord compression and canal stenosis after cervical spine trauma: a study of interrater and intrarater reliability. Spine (Phila Pa 1976) 32(19):2083–2091
Miyanji F, Furlan JC, Aarabi B, Arnold PM, Fehlings MG (2007) Acute cervical traumatic spinal cord injury: MR imaging findings correlated with neurologic outcome—prospective study with 100 consecutive patients. Radiology 243(3):820–827
Kulkarni MV, McArdle CB, Kopanicky D et al (1987) Acute spinal cord injury: MR imaging at 1.5 T. Radiology 164(3):837–843
Book Breiman L, Friedman J, Stone C et al (1984) Classification and regression trees. Chapman and Hall, London
Kelley A, Garshick E, Gross ER, Lieberman SL, Tun CG, Brown R (2003) Spirometry testing standards in spinal cord injury. Chest 123(3):725–730
Ditunno JF, Little JW, Tessler A, Burns AS (2004) Spinal shock revisited: a four-phase model. Spinal Cord 42(7):383–395
Dohoo IR, Ducrot C, Fourichon C (1997) An overview of techniques for dealing with large numbers of independent variables in epidemiologic studies. Prev Vet Med. 29(3):221–239
Winslow C, Bode RK, Felton D, Chen D, Meyer PR Jr (2002) Impact of respiratory complications on length of stay and hospital costs in acute cervical spine injury. Chest 121(5):1548–1554
Tator CH (1994) Ischemia as a secondary neural injury. In: Salzman SK, Faden AI (eds) Neurobiology of central nervous system trauma. Oxford University Press, New York, pp 209–215
Roquilly A, Seguin P, Mimoz O et al (2014) Risk factors for prolonged duration of mechanical ventilation in acute traumatic tetraplegic patients—a retrospective cohort study. J Crit Care 29(2):313.e7–313.e13
Aarabi B, Harrop JS, Tator CH et al (2012) Predictors of pulmonary complications in blunt traumatic spinal cord injury. J Neurosurg Spine 17(1 Suppl):38–45
Acknowledgments
No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Conflict of interest
There is no actual or potential conflict of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Y. F. Hou and Y. Lv contributed equally to the paper.
Rights and permissions
About this article

Cite this article
Hou, Y.F., Lv, Y., Zhou, F. et al. Development and validation of a risk prediction model for tracheostomy in acute traumatic cervical spinal cord injury patients. Eur Spine J 24, 975–984 (2015). https://doi.org/10.1007/s00586-014-3731-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3731-y