
Abstract

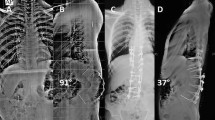
Childhood spinal tuberculosis, especially when associated with severe vertebral destruction of more than two vertebral bodies can end up in severe deformity. These children show progressive deformity throughout the period of growth and can develop severe kyphosis of >100°. Such kyphosis is severely disabling with significant risk of neurological deficit and respiratory compromise. Surgical correction of these deformities by both anterior and posterior approaches has been described but each have serious limitations of approach, correctability and safety. We describe here a technique of posterior closing–anterior opening osteotomy, which allowed us to correct a rigid post-tubercular deformity of 118° in a 13-year-old boy with neglected spinal tuberculosis. The patient was a 13-year-old boy, who had contracted spinal tuberculosis at the age of 6 years. Although the disease was cured by anti-tubercular chemotherapy, he continued to deteriorate in deformity and presented to us with severe thoracolumbar kyphosis (118°). He was neurologically intact but was beginning to show shortness of breath on exertion. Patient also had fore shortening of the trunk with impingement of the rib cage on the iliac crest. Radiographs revealed complete destruction of T12, L1 and L2 vertebral bodies with the T11 vertebra fusing with L3 anteriorly. CT scans and MRI revealed severe collapse of the vertebral column and the spinal cord being stretched over the ‘internal gibbus’, which was formed by the remnants of the destroyed vertebrae. A single stage closing–opening osteotomy was done by a midline posterior approach with continuous intraoperative spinal cord monitoring. The procedure involved extensive laminectomy of T11–L2, pedicle screw fixation of three levels above and three levels below the apex, a wedge osteotomy at the apex of the deformity from both sides, anterior column reconstruction by appropriate-sized titanium cage and gradual correction of deformity by closing the posterior column using the cage as a fulcrum. This allowed us to achieve a correction to 38° (68% correction). There was no intraoperative or perioperative adverse event and patient had good functional and radiological outcome at 1-year follow-up. In this Grand Rounds case presentation, we have also discussed the aetiology and evolution of severe post-tubercular kyphosis, which is the most common cause of spinal deformity in the developing world. Early identification of children at risk for severe deformity, the time and ideal methods of prevention of such deformities are discussed. The pros and cons of the available options of surgical correction of established deformity and the merits of our surgical technique are discussed.






Similar content being viewed by others


References
Altman GT, Altman DT, Frankovitch KF (1996) Anterior and posterior fusion for children with tuberculosis of the spine. Clin Orthop 325:225–231
Benli IT, Acaroglu E, Akalin S et al (2003) Anterior radical debridement and anterior instrumentation in tuberculosis spondylitis. Eur Spine J 12:224–234
Bezer M, Kucukdurmaz F et al (2007) Transpedicular decancellation osteotomy in the treatment of posttuberculous kyphosis. J Spinal Disord Tech 20:209–215
Kawahara N, Tomita K, Hisatoshi B et al (2001) Closing–opening wedge osteotomy to correct angular kyphotic deformity by a single posterior approach. Spine 26:391–402
Lonstein JE (1987) Cord compression. In: Bradford DS, Lonstein JE, Ogilvie JW et al (eds) Moe’s textbook of scoliosis and other spinal deformities, 2nd edn. WB Saunders, Philadelphia, pp 540–547
Medical Research Council (1998) A 15-year assessment of controlled trials of the management of tuberculosis of the spine in Korea and Hong Kong: thirteenth report. J Bone Joint Surg Br 80B:456–462
Moon MS, Woo YK, Lee KS et al (1995) Posterior instrumentation and anterior interbody fusion for tuberculous kyphosis of dorsal and lumbar spines. Spine 20:1910–1916
Moon MS (1997) Tuberculosis of the spine, controversies and a new challenge. Spine 22:1791–1797
Moon MS, Kim I, Woo YK, Park YO (1987) Conservative treatment of tuberculosis of the thoracic and lumbar spine in adults and children. Int Orthop 11:315–322
Moon MS, Lee MK (1971) The changes of the kyphosis of the tuberculous spine in children following ambulant treatment. Korean Orthop Assoc 6:203–208
Parathasarathy R, Sriram K, Satha T et al (1999) Short course chemotherapy for tuberculosis of the spine: a comparison between ambulant treatment and radical surgery—10 year report. J Bone Joint Surg 81B:464–471
Rajasekaran S (2002) The problem of deformity in spinal tuberculosis. Clin Orthop 398:85–92
Rajasekaran S (2001) The natural history of childhood spinal tuberculosis: a 15-year prospective study. J Bone Joint Surg Br 83B:954–962
Rajasekaran S, Shanmugasundaram TK (1987) Prediction of the angle of gibbus deformity in tuberculosis of the spine. J Bone Joint Surg Am 69-A(4):503–509
Rajasekaran S (2007) Buckling collapse of the spine in childhood spinal tuberculosis. Clin Orthop 460:86–92
Reyes-Sanchez A, Rosales LM, Miramontes VP et al (2002) Treatment of thoracolumbar fractures by vertebral shortening. Eur Spine J 11:8–12
Suk SI, Kim JH, Lee SM et al (2003) Anterior-posterior surgery versus posterior closing wedge osteotomy in posttraumatic kyphosis with neurologic compromised osteoporotic fracture. Spine 28:2170–2175
Siata K, Hoshini Y, Kikkawa I et al (2000) Posterior spinal shortening for paraplegia after vertebral collapse caused by osteoporosis. Spine 25:2832–2835
Tuli SM (1995) Severe kyphotic deformity in tuberculosis of the spine. Int Orthop 19:327–331
Tuli SM (1991) Tuberculosis of the skeletal system, 3rd edn. Jaypee Brothers, New Delhi
Yau ACMC, Hsu LCS, O’Brien JP, Hodgson AR (1974) Tuberculosis kyphosis-correction with spinal osteotomy, halo-pelvic distraction and anterior and posterior fusion. J Bone Joint Surg 56A:1419–1434
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary video 1 (wmv 18,703 kb)
Rights and permissions
About this article
Cite this article
Rajasekaran, S., Rishi Mugesh Kanna, P. & Shetty, A.P. Closing–opening wedge osteotomy for severe, rigid, thoracolumbar post-tubercular kyphosis. Eur Spine J 20, 343–348 (2011). https://doi.org/10.1007/s00586-010-1526-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-010-1526-3