
Abstract
Purpose
Effective postoperative pain management is important for older surgical patients because pain affects perioperative outcomes. A prospective cohort study was conducted to describe the direct and indirect effects of patient risk factors and pain treatment in explaining levels of postoperative pain in older surgical patients.
Methods
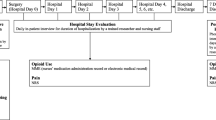
We studied patients who were 65 years of age or older and were scheduled for major noncardiac surgery with a postoperative hospital stay of at least 2 days. The numeric rating scale (0 = no pain, 10 = worst possible pain) was used to measure pain levels before surgery and once daily for 2 days after surgery. Path analysis was performed to examine the association between predictive variables and postoperative pain levels.
Results
Three hundred fifty patients were studied. We found that preoperative pain level, use of preoperative opioids, female gender, higher ASA physical status, and postoperative pain control methods were the strongest predictors of postoperative pain as measured on the first day after surgery. Younger age, greater preoperative symptoms of depression, and lower cognitive function also contributed to higher postoperative pain levels. Pain levels on the second day after surgery were strongly predicted by preoperative pain level, use of preoperative opioids, surgical risk, and pain and opioid dose on postoperative day 1. However, younger age, female gender, higher ASA physical status, greater preoperative symptoms of depression, lower cognitive function, and postoperative pain control methods indirectly contributed to pain levels on the second day after surgery.
Conclusion
Although preoperative pain and use of preoperative opioids have the strongest effects on postoperative pain, clinicians should be aware that other factors such as age, gender, surgical risk, preoperative cognitive impairment, and depression also contribute to reported postoperative pain. Based on significant statistical correlations, these study results can contribute to more effective postoperative care for those patients having the risk factors studied here. Preoperative treatment/intervention based in part on factors such as preoperative pain, use of preoperative opioids, and depression may improve postoperative pain management.


Similar content being viewed by others


References
Berry PH, Dahl JL. The new JCAHO pain standards: implications for pain management nurses. Pain Manag Nurs. 2000;1:3–12.
Liu SS, Wu CL. Effect of postoperative analgesia on major postoperative complications: a systematic update of the evidence. Anesth Analg. 2007;104:689–702.
Puntillo K, Weiss SJ. Pain: its mediators and associated morbidity in critically ill cardiovascular surgical patients. Nurs Res. 1994;43:31–6.
Rodgers A, Walker N, Schug S, McKee A, Kehlet H, van Zundert A, Sage D, Futter M, Saville G, Clark T, MacMahon S. Reduction of postoperative mortality, morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321:1493.
Vaurio LE, Sands LP, Wang Y, Mullen EA, Leung JM. Postoperative delirium: the importance of pain and pain management. Anesth Analg. 2006;102:1267–73.
Poleshuck EL, Katz J, Andrus CH, Hogan LA, Jung BF, Kulick DI, Dworkin RH. Risk factors for chronic pain following breast cancer surgery: a prospective study. J Pain. 2006;7:626–34.
Peters ML, Sommer M, de Rijke JM, Kessels F, Heineman E, Patijn J, Marcus MA, Vlaeyen JW, van Kleef M. Somatic and psychologic predictors of long-term unfavorable outcome after surgical intervention. Ann Surg. 2007;245:487–94.
Eagle KA, Berger PB, Calkins H, Chaitman BR, Ewy GA, Fleischmann KE, Fleisher LA, Froehlich JB, Gusberg RJ, Leppo JA, Ryan T, Schlant RC, Winters WL Jr, Gibbons RJ, Antman EM, Alpert JS, Faxon DP, Fuster V, Gregoratos G, Jacobs AK, Hiratzka LF, Russell RO, Smith SC Jr. ACC/AHA Guideline Update for Perioperative Cardiovascular Evaluation for Noncardiac Surgery—executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1996 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Anesth Analg. 2002;94:1052–64.
Caumo W, Schmidt AP, Schneider CN, Bergmann J, Iwamoto CW, Adamatti LC, Bandeira D, Ferreira MB. Preoperative predictors of moderate to intense acute postoperative pain in patients undergoing abdominal surgery. Acta Anaesthesiol Scand. 2002;46:1265–71.
Kalkman CJ, Visser K, Moen J, Bonsel GJ, Grobbee DE, Moons KG. Preoperative prediction of severe postoperative pain. Pain. 2003;105:415–23.
De Cosmo G, Congedo E, Lai C, Primieri P, Dottarelli A, Aceto P. Preoperative psychologic and demographic predictors of pain perception and tramadol consumption using intravenous patient-controlled analgesia. Clin J Pain. 2008;24:399–405.
Gagliese L, Gauthier LR, Macpherson AK, Jovellanos M, Chan VW. Correlates of postoperative pain and intravenous patient-controlled analgesia use in younger and older surgical patients. Pain Med. 2008;9:299–314.
Bijur PE, Latimer CT, Gallagher EJ. Validation of a verbally administered numerical rating scale of acute pain for use in the emergency department. Acad Emerg Med. 2003;10:390–2.
Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, Leirer VO. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17:37–49.
Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry. 1999;14:858–65.
Ferrucci L, Del Lungo I, Guralnik JM, Bandinelli S, Benvenuti E, Salani B, Lamponi M, Ubezio C, Benvenuti F, Baroni A. Is the telephone interview for cognitive status a valid alternative in persons who cannot be evaluated by the Mini Mental State Examination? Aging (Milano). 1998;10:332–8.
Marcantonio ER, Goldman L, Mangione CM, Ludwig LE, Muraca B, Haslauer CM, Donaldson MC, Whittemore AD, Sugarbaker DJ, Poss R, Haas S, Cook EF, Orav EJ, Lee TH. A clinical prediction rule for delirium after elective noncardiac surgery. JAMA. 1994;271:134–9.
Stage FK, Carter HC, Nora A. Path analysis: an introduction and analysis of a decade of research. J Educ Res. 2004;98(1):5–12.
Thomas T, Robinson C, Champion D, McKell M, Pell M. Prediction and assessment of the severity of post-operative pain and of satisfaction with management. Pain. 1998;75:177–85.
Gramke HF, de Rijke JM, van Kleef M, Kessels AG, Peters ML, Sommer M, Marcus MA. Predictive factors of postoperative pain after day-case surgery. Clin J Pain. 2009;25:455–60.
Wilder-Smith OH, Tassonyi E, Arendt-Nielsen L. Preoperative back pain is associated with diverse manifestations of central neuroplasticity. Pain. 2002;97:189–94.
Chung F, Ritchie E, Su J. Postoperative pain in ambulatory surgery. Anesth Analg. 1997;85:808–16.
Ip HY, Abrishami A, Peng PW, Wong J, Chung F. Predictors of postoperative pain and analgesic consumption: a qualitative systematic review. Anesthesiology 2009;110(5):1061–1067.
Cole LJ, Farrell MJ, Gibson SJ, Egan GF. Age-related differences in pain sensitivity and regional brain activity evoked by noxious pressure. Neurobiol Aging 2010;31(3):494–503 (e-pub 2008).
Ochsner KN, Ludlow DH, Knierim K, Hanelin J, Ramachandran T, Glover GC, Mackey SC. Neural correlates of individual differences in pain-related fear and anxiety. Pain. 2006;120:69–77.
Acknowledgments
This work was supported in part by the Anesthesia Patient Safety Foundation (Indianapolis, IN)/Anesthesia Healthcare Partners Research Award (JML) and NIH Grant [5RO1AG31795-02] (JML). Presented in part at the annual meeting of the American Society of Anesthesiologists, Las Vegas, October 2005.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1
High-risk surgery
-
1.
Aortic vascular surgery
-
2.
Peripheral vascular surgery
-
3.
Prolonged procedures associated with large fluid shifts or blood loss (any intraabdominal procedures such as bowel resection, which is 6 h in duration, other than appendectomy; any procedures with blood loss >1,000 ml; radical cystectomy with ileal loop) are high risk.
Intermediate-risk surgery
-
1.
Carotid endarterectomy
-
2.
Head and neck surgery (ear–nose–throat surgery)
-
3.
Intraperitoneal and intrathoracic surgeries (total pneumonectomy is high risk; lobectomy and partial lung resection are intermediate risk)
-
4.
Prostate surgery (TURP and radical prostatectomy except when the latter involves large blood loss as defined previously)
-
5.
Orthopedic surgery
-
6.
One- to two-level laminectomies (multiple levels with spinal fusion with blood loss >1,000 ml are high risk)
-
7.
Craniotomies with blood loss <1,000 ml, parotidectomy, radical neck dissection, and parathyroidectomy.
Low-risk surgery
-
1.
Breast surgery
-
2.
Plastic surgery
-
3.
Any “superficial” surgeries, including voice prosthesis; inguinal hernia; endoscopic surgeries.
Appendix 2
Standardized direct and indirect effects on pain and opioid dose
Effect | Direct | Indirect | Total |
|---|---|---|---|
Pre-op pain | |||
Gender (female) | 0.129* | 0.129* | |
Use of pre-op opioids | 0.262*** | 0.262*** | |
Pre-op TICS over 30 | −0.097+ | −0.097+ | |
Geriatric Depression Scale | 0.110* | 0.110* | |
Pain on POD1 | |||
Pre-op pain | 0.206*** | 0.206*** | |
Age over 80 | −0.111* | −0.111* | |
High ASA PS | 0.144** | 0.144** | |
Gender (female) | 0.138** | 0.027* | 0.165*** |
Geriatric Depression Scale | 0.023+ | 0.023+ | |
Use of pre-op opioids | 0.212*** | 0.054** | 0.266*** |
IV-PCA analgesia | 0.125** | 0.125* | |
Pre-op TICS over 30 | −0.020+ | −0.020+ | |
Pain on POD2 | |||
Pre-op pain | 0.260*** | 0.085*** | 0.345*** |
Pain on POD1 | 0.389*** | 0.026* | 0.415*** |
Opioid dose on POD1 | 0.139** | 0.139** | |
Age over 80 | −0.046* | −0.046* | |
Gender (female) | 0.102*** | 0.102*** | |
High ASA PS | 0.060** | 0.060** | |
Geriatric Depression Scale | 0.038* | 0.038* | |
Use of pre-op opioids | 0.179*** | 0.179*** | |
IV-PCA analgesia | 0.097*** | 0.097*** | |
Pre-op TICS over 30 | −0.034+ | −0.034+ | |
High surgical risk | 0.124** | 0.124** | |
Opioid dose on POD1 | |||
Pre-op pain | 0.038** | 0.038** | |
Pain on POD1 | 0.185*** | 0.185*** | |
Age over 80 | −0.021* | −0.021* | |
Gender (female) | 0.030** | 0.030** | |
High ASA PS | 0.027* | 0.027* | |
Geriatric Depression Scale | 0.004+ | 0.004+ | |
Use of pre-op opioids | 0.049** | 0.049** | |
IV-PCA analgesia | 0.327*** | 0.023* | 0.350*** |
Pre-op TICS over 30 | −0.004 | −0.004 | |
Opioid dose on POD2 | |||
Opioid dose on POD1 | 0.518*** | 0.020* | 0.538*** |
Pre-op pain | 0.070*** | 0.070*** | |
Pain on POD1 | 0.156*** | 0.156*** | |
Pain on POD2 | 0.145** | 0.145** | |
Age over 80 | −0.017* | −0.017* | |
Gender (female) | 0.031** | 0.031** | |
High ASA PS | 0.108* | 0.022* | 0.130** |
Geriatric Depression Scale | 0.008+ | 0.008+ | |
Use of pre-op opioids | 0.051*** | 0.051*** | |
IV-PCA analgesia | 0.196*** | 0.196*** | |
Pre-op TICS over 30 | −0.007+ | −0.007+ | |
High surgical risk | 0.018* | 0.018* | |
About this article
Cite this article
Kinjo, S., Sands, L.P., Lim, E. et al. Prediction of postoperative pain using path analysis in older patients. J Anesth 26, 1–8 (2012). https://doi.org/10.1007/s00540-011-1249-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-011-1249-6