
Abstract
Background
Many mildly to moderately obese individuals with a body mass index (BMI) lower than 35 kg/m2 have serious diseases related to their obesity. Nonsurgical therapy is ineffective in the long term, yet surgery has never been made widely available to this population.
Methods
Between 2002 and 2007, 53 patients with a BMI lower than 35 kg/m2 underwent laparoscopic adjustable gastric banding at our institution. Data on all these patients were collected prospectively and entered into an institutional review board–approved electronic registry. The study parameters included preoperative age, gender, BMI, presence of comorbidities, percentage of excess weight loss (%EWL), and resolution of comorbidities.
Results
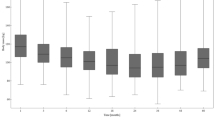
The mean preoperative age of the patients was 46.9 years (range, 16–68 years), and the mean preoperative BMI was 33.1 kg/m2 (range, 28.2–35.0 kg/m2). Of the 53 patients, 49 (92%) had at least one obesity-related comorbidity. The mean BMI decreased to 28.1 ± 2.4 kg/m2, 25.8 ± 2.9 kg/m2, and 25.8 ± 3.1 kg/m2 and mean %EWL was 48.3 ± 17.6, 69.9 ± 28.0, and 69.7 ± 31.7 at 0.5, 1, and 2 years, respectively. Substantial improvement occurred for the following comorbidities evaluated: hypertension, depression, diabetes, asthma, hypertriglyceridemia, obstructive sleep apnea, hypercholesterolemia, and osteoarthritis. There was one slip, two cases of band obstruction (from food), two cases of esophagitis, and two port leaks, but no mortality.
Conclusion
The authors are very encouraged by this series of low-BMI patients who underwent laparoscopic adjustable gastric banding. Their weight loss has been excellent, and their complications have been acceptable. Their comorbidities have partially or wholly resolved. With further study, it is reasonable to expect alteration of the weight guidelines for bariatric surgery to include patients with a BMI lower than 35 kg/m2.



Similar content being viewed by others


References
Ogden CL, Carroll MD, McDowell MA, Flegal KM (2007) Obesity among adults in the United States—no statistically significant change since 2003–2004. NCHS data brief number 1, National Center for Health Statistics, Hyattsville, MD
WHO Consultation on Obesity (1999) Obesity: preventing and managing the global epidemic: report of a WHO consultation, WHO, Geneva, Switzerland
Douketis JD, Macie C, Thabane L, Williamson DF (2005) Systematic review of long-term weight loss studies in obese adults: clinical significance and applicability to clinical practice. Int J Obes Lond 29:1153–1167
Sjostrom L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B, Dahlgren S, Larsson B, Narbro K, Sjostrom CD, Sullivan M, Wedel H, Swedish Obese Subjects Study Scientific Group (2004) Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 351:2683–2693
Consensus Development Conference Panel (1991) Gastrointestinal surgery for severe obesity. Ann Intern Med 115:956–961
Angrisani L, Favretti F, Furbetta F, Iuppa A, Doldi SB, Paganelli M, Basso N, Lucchese M, Zappa M, Lesti G, Capizzi FD, Giardiello C, Di Lorenzo N, Paganini A, Di Cosmo L, Veneziani A, Lacitignola S, Silecchia G, Alkilani M, Forestieri P, Puglisi F, Gardinazzi A, Toppino M, Campanile F, Marzano B, Bernante P, Perrotta G, Borrelli V, Lorenzo M (2004) Italian group for lap-band system: results of multicenter study on patients with BMI ≤ 35 kg/m2. Obes Surg 14:415–418
O’Brien PE, Dixon JB, Laurie C, Skinner S, Proietto J, McNeil J, Strauss B, Marks S, Schachter L, Chapman L, Anderson M (2006) Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program: a randomized trial. Ann Intern Med 144:625–633
Dixon JB, O’Brien PE, Playfair J, Chapman L, Schachter LM, Skinner S, Proietto J, Bailey M, Anderson M (2008) Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA 299:316–323
Ren CJ, Fielding GA (2003) Laparoscopic adjustable gastric banding: surgical technique. J Laparoendosc Adv Surg Tech A 13:257–263
Gulkarov I, Wetterau M, Ren CJ, Fielding GA (2007) Hiatal hernia repair at the initial laparoscopic adjustable gastric band operation reduces the need for reoperation. Surg Endosc 22:1035–1041
Shen R, Dugay G, Rajaram K, Cabrera I, Siegel N, Ren CJ (2004) Impact of patient follow-up on weight loss after bariatric surgery. Obes Surg 14:514–519
Flegal KM, Carroll MD, Ogden CL, Johnson CL (2002) Prevalence and trends in obesity among U.S. adults, 1999–2000. JAMA 288:1723–1727
Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM (2006) Prevalence of overweight and obesity in the united states, 1999–2004. JAMA 295:1549–1555
Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW Jr (1999) Body mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med 341:1097–1105
Fobi M, Lee H, Igwe D, Felahy B, James E, Stanczyk M, Fobi N (2002) Gastric bypass in patients with BMI 32 without life-threatening comorbidities: preliminary report. Obes Surg 12:52–56
Parikh M, Duncombe J, Fielding GA (2006) Laparoscopic adjustable gastric banding for patients with body mass index of ≤35 kg/m2. Surg Obes Relat Dis 2:518–522
Parikh M, Lo H, Chang C, Collings D, Fielding G, Ren C (2006) Comparison of outcomes after laparoscopic adjustable gastric banding in African Americans and whites. Surg Obes Relat Dis 2:607–610, discussion 610–612
Parikh M, Ayoung-Chee P, Romanos E, Lewis N, Pachter HL, Fielding G, Ren C (2007) Comparison of rates of resolution of diabetes mellitus after gastric banding, gastric bypass, and biliopancreatic diversion. J Am Coll Surg 205:631–635
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sultan, S., Parikh, M., Youn, H. et al. Early U.S. outcomes after laparoscopic adjustable gastric banding in patients with a body mass index less than 35 kg/m2 . Surg Endosc 23, 1569–1573 (2009). https://doi.org/10.1007/s00464-009-0341-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-009-0341-6