
Abstract
Purpose
Collecting waste is regarded as a benchmark for “particularly heavy” work. This study aims to determine and compare the workload of refuse workers in the field. We examined heart rate (HR) and oxygen uptake as parameters of workload during their daily work.
Methods
Sixty-five refuse collectors from three task-specific groups (residual and organic waste collection, and street sweeping) of the municipal sanitation department in Hamburg, Germany, were included. Performance was determined by cardiopulmonary exercise testing (CPX) under laboratory conditions. Additionally, the oxygen uptake (VO2) and HR under field conditions (1-h morning shift) were recorded with a portable spiroergometry system and a pulse belt.
Results
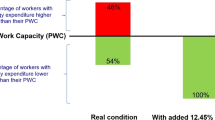
There was a substantial correlation of both absolute HR and VO2 during CPX [HR/VO2 R 0.89 (SD 0.07)] as well as during field measurement [R 0.78 (0.19)]. Compared to reference limits for heavy work, 44 % of the total sample had shift values above 30 % heart rate reserve (HRR); 34 % of the individuals had mean HR during work (HRsh) values that were above the HR corresponding to 30 % of individual maximum oxygen uptake (VO2,max). All individuals had a mean oxygen uptake (VO2,1h) above 30 % of VO2,max.
Conclusion
HR as well as the measurement of VO2 can be valuable tools for investigating physiological workload, not only under laboratory conditions but also under normal working conditions in the field. Both in terms of absolute and relative HR and oxygen consumption, employment as a refuse collector should be classified in the upper range of defined heavy work. The limit of heavy work at about 33 % of the individual maximum load at continuous work should be reviewed.
Similar content being viewed by others

Introduction
The organized collecting of waste is essential for a functioning community; however, there is no explicit job qualification connected with, and the work of garbage collectors receives little scientific attention. Collecting waste is described as physically demanding work and as being the cause of various physical disorders with respiratory, gastrointestinal, and musculoskeletal symptoms (Kuijer and Frings-Dresen 2004; Kuijer et al. 2010). This work is regarded as a benchmark for “particularly heavy” work. The definition of “heavy work” is based so far only on the assumption that the endurance limit is 30 % respectively 33 % of the maximum load capacity, taking into account load peaks, manual work, and harmful temperatures (Ilmarinen et al. 1991; Rutenfranz et al. 1976). The determination of an “upper limit” is essential for defining the “reasonableness” of a work—in the sense of the absence of excessive risks to health. There are presently also no indications, showing how the physical performance is with this heavy work with increasing age. An assessment is required in order to meet the challenges of demographic change in industrialized countries. Only few studies have investigated in detail the refuse collectors in different countries with different tasks. Up to now, the heart rate (HR) is used as an indirect indicator of the physiological workload, for example in the Netherlands (Kemper et al. 1990), Japan (Tsujimura et al. 2012), and Brazil (Anjos et al. 2007). The oxygen uptake (VO2), as a direct measure of the metabolic processes, however, was mostly estimated via HR in these groups. So far, the VO2 of refuse collectors was determined only once by means of simulation in the laboratory (Kemper et al. 1990; Frings-Dresen et al. 1995). The relation between HR and VO2 has not yet been specified under field conditions. This may be due to the fact that the measurement of oxygen uptake with a breathing mask for outdoor work in this occupation group is technically particularly challenging. In our view, however, the conclusion of HR on VO2,max requires a review. To our knowledge, there are no recent studies with refuse collectors, who were investigated during their daily work with portable spiroergometry to determine the real oxygen uptake.
This paper is based on a study about the physiological workload of 65 employees from three task-specific groups [residual waste collection (RWC), organic waste collection (OWC), and street cleaning (SC)] of a municipal sanitation department in Germany. Our aim was to categorize the respective workload of these professions under real working conditions as a contribution to the development of a classification of workload in occupational health research. To evaluate the methods in the field of measurement, we also conducted comparisons of the methods of workload measurement. For this purpose, HR and oxygen uptake were determined in field measurements. For comparison, we measured the oxygen uptake by a stationary cycle cardiopulmonary exercise test (CPX).
Methods
The study group consisted of 65 subjects (62 males and 3 females), aged between 25 and 60, all employees in the municipal sanitation department in Hamburg, Germany. All participants volunteered and were granted compensatory time off by the employer. Before the start of the investigations, there was no selection of participants. The anthropometric characteristics of the subjects (Table 1) are representative in age and sex of the 1544 employees [46.5 (SD 8.6) years; 98 % male) working in refuse collecting in this sanitation department. The examined employees were subdivided by their occupational tasks into three groups: RWC (n = 35), OWC (12), and SC (18). These jobs are mainly performed by male employees, although there are a few females in street sweeping in Hamburg. There were three women in the last group. The Declaration of Helsinki has been adequately addressed, and written informed consent was obtained from all participants. The study was approved by the Ethics Committee of the Hamburg Medical Association (register number PV4524).
Elements of investigation were specific questioning and physical examination (regarding occupation, symptoms, and disorders according to body functions). Furthermore, spirometry, body plethysmography (MasterScreen™ Body by JAEGER™/CareFusion, Hoechberg, Germany), and CPX were performed with 61 subjects. Four persons were excluded due to cardiorespiratory risk factors.
Spirometry represents a measure of forced one-second capacity and vital capacity (FEV1, FVC) performed according to the criteria of the American Thoracic Society (1995) with the calculation of FEV1/FVC. In addition, body plethysmography determines the airways resistance as well as intrathoracic gas volume.
CPX was performed according to the recommendations of the German Society of Pneumology (Meyer et al. 2013) with 12-lead ECG monitoring on an electronically braked computer-controlled cycle ergometer (ergoselect 200p/Ergoline Bitz, Germany) with a continuous increase in the load. This ramp-like protocol enables a precise determination of maximal aerobic and power output and the ventilatory threshold (VT) (Binder et al. 2008; Meyer et al. 2005). Performance and VO2 and carbon dioxide outputs (VCO2) were measured continuously (Oxycon Pro™ by JAEGER™/CareFusion, Hoechberg, Germany).
CPX was preceded by 2 min of sitting at rest. After a warm-up period of 2 min with an external workload of 25 W, the exercise followed with an increase of 15–25 W/min (Meyer et al. 2013) depending on the individual fitness level. Subjects were verbally encouraged until they could no longer sustain the required crank frequency of 60–70 rpm. Maximum oxygen uptake (VO2,max) was calculated as the average of the highest eight consecutive breaths in the final minute of exercise. The standard equations by Hansen et al. (1984), Reiterer (1975), and Wasserman et al. (2004) for VO2,max and maximal wattage (P max) were used for assessment. The VT corresponds to the first VT; it was determined with a combination of VCO2/VO2 slope and increase in minute ventilation (VE) relative to oxygen consumption (VE/VO2), ventilatory equivalent named. This first VT is defined by the increase in VE/VO2 without a concurrent increase in VE/VCO2 (Binder et al. 2008; Westhoff et al. 2013).
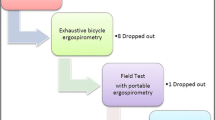
Forty-one subjects were studied while working with long-term HR measurements (T31 coded transmitter, Polar Electro, Buettelborn, Germany) during a work shift (mean 6.7 h). From this group, 20 subjects (18 males and 2 females) were also connected to mobile CPX (Oxycon Mobile by JAEGER™/CareFusion, Hoechberg, Germany) and to the HR monitoring system for an average of 1.3 h to measure the correlation between HR and oxygen uptake under field conditions (HRfield, VO2,field) (Fig. 1). The field measurement was started before the truck left the depot and thus recorded approximately 30 min of driving plus 1 h of sustained work. The actual HR and oxygen uptake under task-specific work were recorded during the following 1 h of continuous work (HR1h, VO2,1h). Part of the work of the garbage collectors is transporting two-wheeled waste containers (120 l volume) of houses and cellars and the shift of large four-wheeled waste containers (240 l) of storerooms. The path length of an entire work day was estimated with a pedometer and was about 7–10 km. All waste containers were emptied machine-supported into the truck (Fig. 2a, b, photographs with waste worker, spiroergo mask, and garbage cans). Occasional waste bags were towed. SC consisted of sweeping waste and leaves, sometimes wet leaves, as well as picking up trash. Due to malfunction of the measuring instruments, refusal, and changes in the organization, valid data were obtained for only 13 of 20 subjects.

Flowchart of the measurements

a, b Refuse collector with spiroergo mask, equipment, and garbage cans
Ahead of the gas exchange measurements in the field via face mask, the mobile CPX unit was volume and gas calibrated. HR and oxygen uptake were both depicted in absolute values and relative to individuals’ maximum values (%HRmax, %VO2,max) and individuals’ values at the VT (%HRVT, %VO2,VT). The difference to maximum values as “reserve values” (%HRR, %VO2,R) was defined as: (HRwork − HRrest)/(HRmax − HRrest) × 100 %, and (VO2,work − VO2,rest)/(VO2,max − VO2,rest) × 100 %, respectively. The HR and VO2 at rest (HRrest,VO2,rest) were calculated from the mean values in the first 2 min of the exercise test and the previously measured resting value.
Statistics
Data are presented as means and standard deviations (SD). To assess the equivalence of linear regression, mean values for Pearson correlation (R), intercept, and slope were determined for each individual. Student’s t test and Wilcoxon test were used to determine whether the mean intercepts and slopes differed from 0 to 1, respectively, and to verify differences between sample characteristics and differences from reference limits. All calculations were performed using IBM SPSS Statistics 22. For all statistical analyses, the null hypothesis was rejected at a probability of p < 0.05.
Results
The 65 subjects of the study group showed only low differences in age and in body mass within the total sample for RWC, OWC, and SC, respectively (Table 1). All 61 subjects who could participate in the CPX had normal ECG readings and took no HR-affecting drugs. On the basis of spirometry and body plethysmography, obstructive lung disease (FEV1/FVC < 70 %) was observed in 21.5 % of subjects. All workers diagnosed with pulmonary disorders were active or former smokers (35.4 and 43.1 % of total sample, respectively).
The results from HR measurement at work (HRsh) of 41 subjects with an average work shift time of 6.7 h are shown in Table 2. Mean values of the total sample were 100.2 b/min and 27.9 % HRR, respectively. The HRsh values relative to individuals’ HRmax and to HRVT (%HRmax, %HRVT) determined in the laboratory CPX showed that the OWC had the highest strain compared with the three subgroups (data not shown in detail).
HR recorded during one representative work hour (Table 3) showed a slightly higher mean HR1h of 109.2 b/min and 45.1 % HRR, respectively, for the 13 subjects (for whom also the oxygen uptake was measured) than in the measurement over the whole work shift of the total sample. There were no significant differences between the groups OWC, RWC, and SC for 1 h of measurement. Mean HR values during 1 h as well as during a work shift were close to the HR at VT. Between HR1h and HRsh of these 13 subjects, there was a mean correlation coefficient of R 0.64. The regression of HR1h was slightly but significantly (p < 0.05) higher than HRsh by 10.6 b/min. During the one representative working hour (Table 3), the group mean achieved an oxygen uptake (VO2,1h) of 1103 ml/min. Here too, mean VO2 was close to VO2,VT. The groups did not differ significantly.
The results of CPX with measurement of VO2 of all 61 participants and of the 13 subjects with field measured data are depicted in Tables 4 and 5. The three subgroups RWC, OWC, and SC do not differ significantly in this test with respect to P max, VO2,max, and HRmax (data not shown). The spiroergometric field measurements’ sample of 13 subjects did not differ significantly from the whole group. A relationship between the maximal values from P max and VO2,max could be observed with mean correlation coefficient (R) of 0.88; HRmax was weakly correlated with age (R 0.45). Therefore, older participants showed surprisingly a slight increase in HRmax with age (data not shown in detail). The individuals reached values close to age-predicted values with 95.6 % (SD 18.2) VO2,max/VO2,pred, and 90.8 % (SD 7.4) HRmax/HRpred, (Hansen et al. 1984; Reiterer 1975; Wasserman et al. 2004).
The linear regression analysis was accomplished to study the relationship between HR and VO2 for CPX and field measurement. Data of HR and oxygen uptake during CPX create an individual linear heart/oxygen uptake relationship and a substantial correlation (mean R 0.89, p < 0.001). There was also a linear regression, with a mean correlation coefficient of R 0.78 (p < 0.001) between HRfield and VO2,field. The equations obtained here were nearly the same; both regressions for CPX and field measurement are shown in Fig. 3a, b. The correlation between %HRR and %VO2,R during CPX was high (R 0.96). The correlation during field measurement was similar, albeit lower, (R 0.78, both p < 0.001) (Fig. 4a, b).

Heart rate (HR) and oxygen uptake (VO2) during CPX with increasing workload by 15–25 W/min (a) and during spiroergometric field measurement at work (b), for 13 subjects. a HR (b/min) = 0.03 × VO2 (ml/min) + 70.95 (drawn trendline); R 2 = 0.80; n = 426; p < 0.001. b. HR (b/min) = 0.03 × VO2 (ml/min) + 76.2 (drawn trendline); R 2 = 0.65; n = 2191; p < 0.001

Heart rate as a percentage of heart rate reserve (%HRR) in relation to oxygen uptake as a percentage of oxygen uptake reserve (%VO2,R), determined during CPX (a) and field measurement (b), for 13 subjects. a %HRR = 0.925 × %VO2,R (ml/min) − 0.017; R 2 = 0.93; n = 325; p < 0.001. b %HRR = 0.783 × %VO2,R (ml/min) + 0.130; R 2 = 0.68; n = 2146; p < 0.001
During the field measurement of continuous HRfield and VO2,field, a simultaneous increase and decrease in HR and oxygen uptake could be observed in each individual. In Fig. 5, a typical example is given of one subject.

Case report: heart rate and oxygen uptake during field measurement (HRfield,VO2,field) of one subject. Individual maximal heart rate, maximal oxygen uptake (HRmax, VO2,max), and the values at ventilatory threshold (HRVT, VO2,VT) are also shown
Discussion
Relationship of HR to VO2 to determine the validity of measuring methods in the field
Heart rate increases linearly as a function of workload intensity and is closely related to oxygen uptake (Arts and Kuipers 1994; Gastinger et al. 2010). Nevertheless, the value of the HR/VO2 relationship can vary between individuals due to metabolic stress or physical training level and therefore should be ascertained individually (Skinner et al. 2003). Similarly, interindividual differences are observed when CPX and field measurements during work are compared. To determine the physiological workload of physically demanding work, we investigated the relation between HR and oxygen uptake under field conditions. We could demonstrate that the HR/VO2 relationship was linear not just during the incremental cycle exercise test (CPX) but also in their usual working environment with climatic and other factors. Nevertheless, the range of the correlation coefficients shows that HR is more strongly correlated to VO2 during CPX (R 0.89, p < 0.001) than during field measurement (R 0.78, p < 0.001) (Fig. 3a, b). Yet, there is a significant correlation between HR and VO2 in the field measurement, and furthermore, a congruent increasing and decreasing profile could be demonstrated (Fig. 5).
Due to different proportions between HR and VO2, a method based on heart rate reserve (%HRR) and VO2 reserve (%VO2,R) is widely used for the comparison of relative values. Swain and Leutholtz (1997) and recent studies by Lounana et al. (2007) have shown that %HRR data at group level are consistent with %VO2,R. We aimed to find out whether this correlation can also be validated for our group in CPX and especially in spiroergometric field measurement under working conditions. For the incremental exercise testing, we can confirm a substantial correlation of %HRR and %VO2,R with R 0.96 (p < 0.01) (Fig. 4a). For spiroergometric field measurement, we found a lower correlation of R 0.78 (p < 0.001). Both regressions show that %HRR does not overestimate %VO2,R as their intercepts are close to 0 (Fig. 4b). Possible reasons for lower field correlations between HR and VO2 could be malfunctioning in gathering the individual values, different load shapes, and the varyingly high intensity of physical strain of muscle groups with differing efficiency. During work as a refuse collector, especially arm work is performed, while the incremental cycle exercise consists mostly of legwork. A better equivalence between %HRR and %VO2,R for legwork than for arm work has been described by (Rotstein and Meckel 2000). Additionally, HR can be impaired by further factors, such as temperature, emotion, and physical fitness status (Achten and Jeukendrup 2003). We nevertheless could demonstrate an equivalence between absolute values of HR and VO2, and equally in relative calculations to HRR and VO2,R in dynamic work, even if it was measured in the field.
Fitness and workload capacity evaluated by various thresholds and aspects
Because the VT reflects the workload threshold beyond which endurance exercise will not lead to anaerobic metabolism, it can therefore be regarded as the upper limit of intensity during the endurance performance (Binder et al. 2008). The present study showed a high endurance performance for the entire sample during 1 h of work and also during the whole work shift, depending on the HR measurement with a mean of 86.7 % HRVT and 79.4 % HRVT, respectively. The percentage of VO2 during 1 h of work in percentage of VO2,VT was likewise, but lower, with a mean of 60 % VO2,VT. In Fig. 5, which shows a representative measurement from the field tests, the subject’s HR well exceeded most of the time the individual HRVT. Similarly, VO2,VT was exceeded several times. For individual values relative to the VT (%HRVT, %VO2,VT), our data show that %HRVT may overestimate the real workload; %VO2,VT seems to be more realistic (see Table 5). Furthermore, VT not only differs between individuals but also varies depending on the state of training and the type of exercise protocol (Faude et al. 2009). Therefore, the question arises whether %HRVT is comparable to %VO2,VT. We would recommend to determine VT and likewise the HRVT and VO2,VT, by CPX in the laboratory. This will enable an accurate estimate of %VO2,VT during the field measurement.
In our sample, the CPX results are close to the individual predicted and age-dependent values (Table 2). Kroidl et al. (2014) have described the requirements for high, normal, and pathological endurance performance, based on values at VT > 80 %, around 60 %, and <40 % of maximal values, respectively. In comparison, our subjects also reached performance levels in the upper range of normal endurance (Table 2). In the present study, workers show normal ranges of individual fitness. Long work periods with a high level of physical activity did not lead to an increase in maximal oxygen uptake, and only slightly better endurance performance was observed in them. This seems to be compatible with results from previous studies which also investigated workers with heavy workload (Ilmarinen et al. 1991; Søgaard et al. 1996).
It is commonly suggested that 33–40 % of the individual’s VO2,max should be the capable workload for 8 h of physical work (Åstrand et al. 2003; Ilmarinen 1992). But %VO2,max depends on the type of exercise performed. According to Kemper et al. (1990), the acceptable limit for refuse collecting work in particular, which mainly consists of arm work combined with legwork, should be at 30 % VO2,max for an 8-h shift. To describe the exercise intensity in our sample, we took HRsh at a given %VO2,max. This method is according to Skinner et al. (2003); they have demonstrated that once VO2,max and the relationship among HR and VO2 are known, the corresponding HR is a good estimate for relative workload. Taking the mean HR values of the 41 subjects in our study who had undergone HRsh measurement, there was a slight exceedance (mean HR 100.2 b/min) of the standards of calculated mean HR value at 30 % VO2,max (96.6 b/min); ns). Here, 66 % of the individuals had mean HRsh values above 30 % VO2max. Frings-Dresen and Kemper 1995, under laboratory conditions, showed that 33–59 % of the subjects, depending on the waste collector activity (bags, different container volumes), exceeded the 30 % of VO2max.
Comparing these results with the oxygen uptake of the 13 individuals from the 1-h VO2 measurement, the means even exceeded the reference of 30 % VO2,max significantly (mean VO2,1h 1103 ml/min vs. calculated VO2 at 30 % VO2,max of 737.3 ml/min, p < 0.05). All subjects achieved a mean VO2, which was above the reference limit of 30 % VO2,max, with a total range of 35–69 % VO2,max. These results are consistent with the relation between HR1h and HRsh as the 1-h values were slightly but significantly higher than HRsh. Nevertheless, in both specifications (HR and VO2), very high values have been found, which reflects the high continuous work load of refuse collectors.
In general, exercises that are performed with a HRR > 30 % for an 8-h shift are assumed to be at high cardiovascular load (Ilmarinen et al. 1991; Shimaoka et al. 1998). With long-term HR measurement for a work shift of 6.7 h, 39 % of residual waste collectors, 33 % of organic waste collectors, and 39 % of the street cleaners had %HRR,sh values that were higher than 30 % HRR. These findings are consistent with Kuijer et al. (1999), who found 36.4 %HRR for refuse collectors and 22.6 %HRR for street sweepers. Therefore, we can conclude that refuse collectors and street cleaners have high endurance performance and high cardiovascular load during work.
Åstrand et al. (2003) specified easy, moderate, and heavy work during an 8-h work shift on the basis of oxygen consumption at <600, 600–1000, and >1000 ml/min VO2, respectively, and required a maximum VO2 for work at 40 %VO2,max at <1500, <1500–2500, and >2500 ml/min, respectively. When compared to Åstrand’s requirements of workload, the refuse collectors in our study had a mean VO2,1h of 1103 ml/min during work corresponding to 46 % VO2,max (Table 4) and a mean VO2,max of 2623 ml/min during CPX corresponding to oxygen uptake under heavy physical work. This confirms Åstrand’s findings; the workload of refuse collectors can be classified in the upper field of heavy work. Whether the relatively high physical endurance is a health risk for the refuse collectors remains open. In our initial cross-sectional study, we found no evidence to this.
Comparison with other occupations
Compared to jobs which are commonly referred to as physically heavy, the relative workload found in this study was rather high. The means for HRsh and %HRmax (Table 3) during one work shift are consistent with Wultsch et al. (2012) findings for workers from waste processing (activities were not differentiated). They found mean HRsh 100 b/min for male and 120 for female, 59 and 65 % HRmax, respectively. Compared to the other investigated professions (workers in metal industry, slaughterhouse work, or healthcare business) referred in this study (Wultsch et al. 2012), our findings on the physical demand of refuse collectors were higher. Compared to a study with housekeepers which also used a portable spiroergometric system for field measurements (MJ Fröhlich, personal communication), we found similar values at HR1h and VO2,1h to those they determined with 112 b/min and 1.06 l/min, respectively. However, compared to portable spiroergometric measurements with lumberjacks (Hagen et al. 1993)—their job is considered to be the hardest form of physical work (with 49 % VO2,max for the younger, 53 % VO2,max for the older, and a HRsh of 138 and 126 b/min, respectively)—our measurement results were rather low.
Other studies with refuse collectors have also reported similar HR values to those found in our study. Kemper et al. (1990) have found a mean HRsh of 99.5 b/min in Dutch refuse collectors during one work shift, and—compared to the threshold value of 30 % VO2,max calculated over HRsh—30 % of their participants had exceeded that limit. Furthermore, they also established a linear relationship between HR and VO2 during work, but they did not describe this correlation further. In a recent study with Brazilian refuse collectors, Anjos et al. (2007) outlined a mean HR for the total working time at 97.6 b/min, 53.4 % HRmax, and 32.8 % HRR; nevertheless, their results were partially lower than those found in the present study. In addition, they identified HR values during the actual working time which can be compared with our values for 1 h of continuous work. A recent Japanese study by Tsujimura et al. (2012) found mean HR values for garbage collectors of 97.5 b/min, which were similar to the Brazilians but lower than our findings. These studies of refuse collectors, however, determined the workload only by the HR without VO2 field measurements.
Conclusion
The present study demonstrates that HR and oxygen consumption are strongly correlated even during field measurements of the heavy dynamic work of the refuse collectors. Therefore, HR measurement is a valuable tool for evaluating the parameters of physiological workload during work. But the correlation between HR and VO2 was stronger under steady conditions in the laboratory, while HR can also be influenced by several external circumstances. In addition, we included only persons without heart disease or medication. In persons with cardiac disease or HR influencing medication, the sole determination of HR cannot replace the measurement of VO2. Therefore, if possible, the determination of VO2 should be aimed in the field measurement.
Refuse collectors exceed the upper limits set for physical work stress in the literature (Åstrand et al. 2003; Ilmarinen et al. 1991; Shimaoka et al. 1998). But all investigated employees were in our study within their individual reference limits of physical capacity and aerobic fitness, both in terms of absolute and relative HR as well as in oxygen consumption. The three task-specific groups (RWC, OWC, SC) did not differ in workload. The results of the present study can finally confirm the high workload of refuse collectors with the determination of VO2 at work. In addition, the endurance workload of refuse collectors is well above the hitherto recommended limits. The currently applicable limits for an 8-h shift with a maximum of 33–40 % of the individual’s VO2 max or HRR > 30 % should be reviewed. Other field measurements with determination of oxygen uptake with other physically hardworking professionals are necessary.
References
Achten J, Jeukendrup AE (2003) Heart rate monitoring: applications and limitations. Sports Med 33(7):517–538
American Thoracic Society (1995) Standardization of spirometry. Am J Respir Crit Care Med 152:1107–1136
Anjos LA, Ferreira JA, Damiao JJ (2007) Heart rate and energy expenditure during garbage collection in Rio de Janeiro, Brazil. Cad Saude Publica 23(11):2749–2755
Arts FJ, Kuipers H (1994) The relation between power output, oxygen uptake and heart rate in male athletes. Int J Sports Med 15(5):228–231
Åstrand PO, Rodahl K, Dahl HA, Stromme SB (2003) Textbook of work physiology: physiological bases of exercise, 4th edn. Human Kinetics Publishers, Champaign, II
Binder RK, Wonisch M, Corra U, Cohen-Solal A, Vanhees L, Saner H, Schmid JP (2008) Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur J Cardiovasc Prev Rehabil 15(6):726–734
Faude O, Kindermann W, Meyer T (2009) Lactate threshold concepts: how valid are they? Sports Med 39(6):469–490
Frings-Dresen MHW, Kemper HCG, Stassen ARA, Crolla IFAM, Markslag AMT (1995) The daily workload of refuse collectors working with three different collecting methods: a field study. Ergonomics 38:2045–2055
Gastinger S, Sorel A, Nicolas G, Gratas-Delamarche A, Prioux J (2010) A comparison between ventilation and heart rate as indicator of oxygen uptake during different intensities of exercise. J Sports Sci Med 9(1):110–118
Hagen KB, Vik T, Myhr NE, Opsahl PA, Harms-Ringdahl K (1993) Physical workload, perceived exertion, and output of cut wood as related to age in motor-manual cutting. Ergonomics 36(5):479–488
Hansen JE, Sue DY, Wasserman K (1984) Predicted values for clinical exercise testing. Am Rev Respir Dis 129(2 Pt 2):S49–S55
Ilmarinen J (1992) Job design for the aged with regard to the decline in their maximal aerobic capacity: part I D guidelines for the practitioner. Int J Ind Ergon 10:53–63
Ilmarinen J, Louhevaara V, Korhonen O, Nygard CH, Hakola T, Suvanto S (1991) Changes in maximal cardiorespiratory capacity among aging municipal employees. Scand J Work Environ Health 17(Suppl 1):99–109
Kemper HC, van Aalst R, Leegwater A, Maas S, Knibbe JJ (1990) The physical and physiological workload of refuse collectors. Ergonomics 33(12):1471–1486
Kroidl RF, Schwarz S, Lehnigk B, Fritsch J (2014) Kursbuch Spiroergometrie, 3rd edn. Thieme, Stuttgart
Kuijer PP, Frings-Dresen MH (2004) World at work: refuse collectors. Occup Environ Med 61(3):282–286
Kuijer PP, Visser B, Kemper HC (1999) Job rotation as a factor in reducing physical workload at a refuse collecting department. Ergonomics 42(9):1167–1178
Kuijer PP, Sluiter JK, Frings-Dresen MH (2010) Health and safety in waste collection: towards evidence-based worker health surveillance. Am J Ind Med 53(10):1040–1064
Lounana J, Campion F, Noakes TD, Medelli J (2007) Relationship between %HRmax, %HR reserve, %VO2max, and %VO2 reserve in elite cyclists. Med Sci Sports Exerc 39(2):350–357
Meyer T, Lucia A, Earnest CP, Kindermann W (2005) A conceptual framework for performance diagnosis and training prescription from submaximal gas exchange parameters–theory and application. Int J Sports Med 26(Suppl 1):S38–S48
Meyer FJ, Borst MM, Buschmann HC, Ewert R, Friedmann-Bette B, Ochmann U, Petermann W, Preisser AM, Rohde D, Ruhle KH, Sorichter S, Stahler G, Westhoff M, Worth H (2013) Exercise testing in respiratory medicine. Pneumologie 67(1):16–34
Reiterer W (1975) Methodik eines rektangulären-triangulären Belastungstestes. Herz/Kreisl 7(9):457–462
Rotstein A, Meckel Y (2000) Estimation of %VO2 reserve from heart rate during arm exercise and running. Eur J Appl Physiol 83(6):545–550
Rutenfranz J, Hettinger T, Ilmarinen J, Klimmer F (1976) Beurteilung der Eignung zu schwerer körperlicher Arbeit. In: Drasche H, Essing HG, Florian HJ et al (eds) Ökologischer Kurs: Teil Arbeitsmedizin. Ferdinand Enke, Stuttgart, pp 12–24
Shimaoka M, Hiruta S, Ono Y, Nonaka H, Hjelm EW, Hagberg M (1998) A comparative study of physical work load in Japanese and Swedish nursery school teachers. Eur J Appl Physiol Occup Physiol 77(1–2):10–18
Skinner JS, Gaskill SE, Rankinen T, Leon AS, Rao DC, Wilmore JH, Bouchard C (2003) Heart rate versus %VO2max: age, sex, race, initial fitness, and training response: HERITAGE. Med Sci Sports Exerc 35(11):1908–1913
Søgaard K, Fallentin N, Nielsen J (1996) Work load during floor cleaning: the effect of cleaning methods and work technique. Eur J Appl Physiol Occup Physiol 73(1–2):73–81
Swain DP, Leutholtz BC (1997) Heart rate reserve is equivalent to %VO2 reserve, not to %VO2max. Med Sci Sports Exerc 29(3):410–414
Tsujimura H, Taoda K, Kitahara T (2012) A field study on the physiological workload of garbage collectors in the Japanese summer. Ind Health 50(6):556–566
Wasserman K, Hansen JE, Sue DY, Stringer WW, Whipp BJ (2004) Principles of exercise testing and interpretation, 4th edn. Lippincott Raven, Baltimore
Westhoff M, Ruhle KH, Greiwing A, Schomaker R, Eschenbacher H, Siepmann M, Lehnigk B (2013) Positional paper of the German working group “cardiopulmonary exercise testing” to ventilatory and metabolic (lactate) thresholds. Dtsch Med Wochenschr 138(6):275–280
Wultsch G, Rinnerhofer S, Tschakert G, Hofmann P (2012) Governmental regulations for early retirement by means of energy expenditure cut offs. Scand J Work Environ Health 38(4):370–379
Acknowledgments
The authors would like to thank L. Herrmann, Stadtreinigung, Hamburg, for his support in recruiting the volunteers, and H.-J. Krankenhagen and A. Frosch for preparing heart rate data in the field measurements. We would like to thank Sabine Bößler and Anne Winkelmann for their excellent support with the technical patient examinations. We are indebted to Cordula Bittner, MD, and Thomas von Münster, MD, who implemented clinical examinations. The study is a part of the investigation: “Ergonomic study of waste collectors in the system garbage collection and street cleaning of the municipal sanitation department in Hamburg” and was funded by a grant from Stadtreinigung, Hamburg.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standard
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Declaration of Helsinki 1964 and its later amendments or comparable ethical standards.
Author information
Authors and Affiliations
Corresponding author
Additional information
Alexandra M. Preisser and Linfei Zhou are equally contributing first authors.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Preisser, A.M., Zhou, L., Garrido, M.V. et al. Measured by the oxygen uptake in the field, the work of refuse collectors is particularly hard work: Are the limit values for physical endurance workload too low?. Int Arch Occup Environ Health 89, 211–220 (2016). https://doi.org/10.1007/s00420-015-1064-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-015-1064-8