
Abstract
The purpose of the study was to analyse the influence of HPV infection on the outcome of a randomized clinical trial of conventional (CF) versus 7-days-a-week postoperative radiotherapy (p-CAIR) for squamous cell cancer of the head and neck (SCCHN). Between 2001 and 2004, 279 patients with high-risk SCC of the larynx or cancer of the oral cavity/oropharynx were randomized to receive 63 Gy in fractions of 1.8 Gy given 5 days a week or 7 days a week (Radiother Oncol 87:155–163, 2008). The presence of HPV DNA in 131 archival paraffin blocks was assessed with multiplex quantitative real-time PCR using five consensus primers for the conservative L1 region and molecular beacon probes targeting 14 high-risk HPV subtypes. Following the RT-PCR procedure, we could determine the presence and type of HPV16, HPV18 and the other 12 less frequent oncogenic subtypes. Out of 131 samples, 9 were positive for HPV infection (6.9%), all of them with HPV16 subtype. None of the 65 laryngeal tumours was HPV positive. The 5-year LRC in HPV-positive patients was 100%, compared to 58% in the HPV-negative group (p = 0.02, log-rank test). Amongst 122 patients with HPV-negative tumours, 5-year LRC was 50.3% in p-CF versus 65.2 in p-CAIR (p = 0.37). HPV infection was associated with low expression of EGFR and cyclin D. This study demonstrates a favourable outcome for HPV-positive patients with SCCHN treated with postoperative radiotherapy. While considering the small number of HPV+ tumours, the data set can be considered as hypothesis generating only, the outcome raises new questions on the necessity of aggressive postoperative treatment in HPV+ patients.
Similar content being viewed by others


Introduction
Several recent studies have shown that HPV-positive squamous cell cancer of the head and neck (SCCHN) has different clinical and histological characteristics and better prognosis than HPV-negative tumours [1–4]. The prognostic potential of HPV infection with distinct reference to postoperative radiotherapy has been, however, less frequently addressed. Also, the incidence of HPV infection appears dissimilar in diverse regions of the world and, apparently, changes over time, thus providing background for further research [5, 6]. This prompted us to analyse the HPV infection status of tumour samples obtained from participants of a recently conducted randomized trial on conventional versus accelerated 7-days-a-week postoperative radiotherapy [7] and assess the impact of HPV infection on the outcome of the trial.
Materials and methods
Clinical background of the study
The p-CAIR trial was performed between 2001 and 2004, and recruited 279 patients with high-risk squamous cell cancer of the larynx (158 patients) or cancer of the oral cavity/oropharynx (121 patients). Clinical characteristics of the whole group of 279 patients, a detailed presentation of the risk assessment scale, treatment description and the clinical outcome have been presented elsewhere [7]. Importantly, the patients were randomized to receive 63 Gy in fractions of 1.8 Gy given either 5 days a week (140 patients, p-CF: postoperative conventional fractionation) or 7 days a week (139 patients, p-CAIR: postoperative continuous accelerated irradiation).
Recently, we have presented an analysis of the immunohistochemically assessed expression of five molecular markers (EGFR, nm23, Ki-67, p53 and cyclin D1) in relation to the outcome of the trial. Of the 279 patients who were enrolled, it was possible to obtain data for the molecular studies on 148 patients [8]. The emerging data on the importance of HPV infection on the outcome of radiotherapy for SCCHN prompted us to expand the analysis and evaluate HPV status in the remaining portions of tumours embedded in paraffin blocks. The follow-up data have been updated in the present study and show the status of the patients as of January 2010. We note that the update does not affect the qualitative outcome of the analysis, because new loco-regional recurrences have not been recorded since the last publication.
Characteristics of the patients
Out of 148 paraffin blocks used in the earlier study [8], it was possible to assess HPV infection status in 131 patients. In ten patients no remaining tumour tissue was present in the blocks and in seven the material was of insufficient quality to get informative PCR results. Table 1 presents the clinical characteristics of 131 patients included in the analysis. The general characteristics of the subgroup analysed in the present study did not differ considerably from that of the population of 279 patients. Importantly, the risk factors for recurrence were evenly distributed between the trial arms. The actual mean overall radiation treatment time amongst 131 patients was 49.0 days (SD ±3.6) in CF versus 35.6 (SD ±7.2) in p-CAIR. Two patients in p-CF and four in p-CAIR received total radiation doses lower than planned, due to deteriorating general performance before or during radiotherapy. Three patients in p-CF received total doses higher than in the protocol due to local/nodal tumour progression during treatment or treatment planning. One patient in p-CAIR arm died before radiotherapy was started. The other 121 patients received 63 Gy in 1.8 Gy fractions. None of the patients received chemotherapy. The analysis, as shown, was performed on intention-to-treat basis.
The analysis of HPV status
Detection of HPV DNA in paraffin-embedded tumour histopathological samples was made using RealTime High Risk HPV test (Abbott Molecular). It is a qualitative test that can detect 14 high-risk HPV types in the same reaction. It can differentiate between HPV16, HPV18 and other less frequent HPV types (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68). The HPV target sequence is located in the conserved L1 region of the viral genome. The reaction mix contained three forward and two reverse primers designed to hybridize to an approximately 150-base HPV consensus region. A pair of primers targeting 136 bases in the human β-globin gene, serving as an internal control, was also included. Detection of amplification products was achieved with the aid of 15 distinct fluorescently labeled probes.
The laboratory procedure consisted of three steps: DNA isolation, reaction assembly and real-time PCR. DNA was isolated from archival paraffin-embedded tumour samples. For each sample, ten 10-μm thick sections were collected in an aseptic manner. They were deparaffinized, rehydrated and digested in two changes of xylene, graded alcohols and Proteinase K 100 µg/ml (Sigma–Aldrich) for 24 h at 56°C, respectively. Next, samples were processed using mSample Preparation SystemDNA (Abbott Molecular) where DNA was immobilized on the surface of magnetic microparticles, purified and eluted ready for amplification. The DNA purity and concentration were evaluated with Nanodrop ND-1000 spectrophotometer. On completion of sample preparation, an amplification master mix was prepared with AmpliTaq Gold, MgCl2 solution and oligonucleotide reagent containing primers, probes and dNTPs. The PCR reaction was then assembled in 96-well optical reaction plate by combining 25 μl of master mix and 400 ng of extracted DNA diluted to a final volume of 25 μl with molecular biology-grade purified water (Water Mol Biol grade DNase RNase and Protease-free, 5Prime). Thermocycling and products detection were carried out in the m2000rt real-time PCR instrument (Abbott Molecular, system based on Applied Biosystems Inc. RT7500 thermocycler).
Negative and positive controls were included in each run to verify that sample processing, amplification and detection steps were performed correctly. The negative control was formulated with DNA containing β-globin sequence and poly-dA:dT as carrier DNA. The positive control contained HPV16, HPV18, HPV58 and β-globin sequences tied to the carrier DNA.
Samples were considered to be positive when C t value for any of the detected HPV type and β-globin was less or equal to the cutoff value of 35. Samples for which β-globin C t value was >35 were considered to be non-informative.
Statistical analysis
Loco-regional failure was defined as the recurrence of cancer at the primary tumour site, within the neck or supraclavicular nodes, and distant metastases as recurrence elsewhere. Survival curves were plotted using Kaplan–Meier method and compared using log-rank test.
Results
HPV status versus clinical outcome
HPV DNA was detected in 9 out of 131 tumour samples (6.9%). In all nine cases, HPV 16 subtype was found. Figure 1 shows the flow diagram of the cases assessed for HPV infections, including reference to the primary tumour site. HPV was not detected in any of the 65 patients with cancer of the larynx or hypopharynx, compared to 9/66 (13.6%) HPV+ cases amongst patients with cancer of the oral cavity or oropharynx. Out of 11 patients with cancer of the tonsil, there were 6 HPV+ tumours (54.5%). The other HPV+ tumours included two cancers of the base of tongue and one with cancer of the retromolar triangle. There were no significant differences in patients’ age between the HPV+ and HPV− groups (median age, 59 vs. 57 years, respectively).

Flow diagram of the cases assessed for HPV infections
Five patients with HPV+ tumours were treated with p-CF, and four with p-CAIR. Figure 2a shows loco-regional tumour control according to HPV status irrespective of fractionation. The 5-year loco-regional tumour control was 100% in HPV+ cases, compared to 58% in HPV− cases (p = 0.02, log-rank test). Amongst 122 patients with HPV− tumours, 5-year LRC was 50.3% in p-CF versus 65.2 in p-CAIR (p = 0.37, Fig. 3).

Loco-regional tumour control (a) and metastases-free survival (b) according to HPV infection in 131 patients from p-CAIR trial (irrespective of fractionation)

Loco-regional tumour control according to fractionation in 122 HPV-negative tumours
None of the nine patients with HPV+ tumours developed distant metastases. Five-year distant metastases-free survival in the HPV− group was 82% (Fig. 2b). Two out of nine patients with HPV+ tumours (22.2%) developed metachronous second cancer (bladder cancer and colorectal cancer) compared to 10/122 (8.2%) in the HPV− group.
HPV infection versus expression of selected molecular markers
Using the data from previously published study on molecular markers [8], it was possible to assess the relationship between HPV infection and immunohistochemically assessed expression of EGFR, nm23, Ki-67, p53 and cyclin D1.
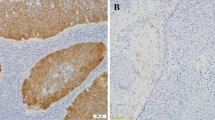
Out of nine HPV+ tumours only one (11%) had high expression of EGFR (more than 33% of the cells stained) compared to 32% in the HPV− group. Also, out of nine HPV+ tumours, only one (11%) had high expression of cyciln D, compared to 29% in the HPV− group. No apparent differences in expression of nm23, Ki-67 or p53 were found between HPV+ and HPV− tumours.
Discussion
Prevalence of HPV infection
Perhaps, the most noticeable result that comes from the present study is that the overall prevalence of HPV infection was low amongst patients enrolled to the p-CAIR trial, at least compared to other recently published studies on this subject [1–3]. Several factors may explain such characteristics of the present group.
The dissimilar rate of infection worldwide is an important factor. In general, the prevalence of HPV in SCCHN is lower in Europe, compared to North America or Asia [5]. Behavioural differences, especially those related to smoking, alcohol consumption, practice of oral sex and number of lifetime sexual partners, may explain the apparent diversity [9]. The majority of patients in the p-CAIR trial inhabited mostly underprivileged, heavily industrialized Upper Silesia region in Poland, characterized by a conservative lifestyle, and high tobacco and alcohol consumption. Such communal characteristics would predispose to HPV-unrelated cancer. Interestingly, the age of patients with HPV+ tumours did not differ from that of the HPV− group in the present study, contrary to many other studies in which HPV-related tumours were detected at a relatively young age [5]. A substantial proportion of patients with cancer of the larynx in the analysed group (65/131, 49.6%) may further contribute to the low prevalence of HPV infection, because HPV+ is more frequent amongst patients with cancer of the oropharynx compared to the larynx. Another factor that contributed to low HPV infection rate was, likely, the selection for p-CAIR trial that accumulated high-risk patients. Also, the prevalence of HPV infection has a propensity to increase with time [6], and would be, likely, higher at present, compared to patients treated between 2001 and 2004. Also, diverse methodological approaches in the assessment of HPV infection may contribute to diversity in the reported prevalence of infection. Most notably, setting different cutoffs for C t value for any of the detected HPV type and β-globin would affect the detection rate.
HPV infection and the outcome of postoperative radiotherapy
Several studies demonstrated that amongst patients with SCCHN, those with HPV+ tumours had a better prognosis than those with HPV− [1–5]. Most of these studies, however, referred to radiotherapy or radiochemotherapy, while the impact of HPV infection on the outcome of postoperative treatment has been less frequently discussed. A small number of HPV+ tumours in the present series preclude definitive conclusions, and the data set can only be used as hypothesis generating. The analysis, nevertheless, suggests that both loco-regional control and metastases-free survival are excellent amongst HPV+ tumours treated with postoperative radiotherapy, though these tumours were originally considered to be at high risk for recurrence according to traditional pathological criteria. Neither loco-regional failures nor distant metastases were observed in long-term follow-up amongst nine individuals with HPV+ tumours irrespective of fractionation. This raises new questions about the necessity of aggressive adjuvant postoperative treatment in HPV+ patients, providing the background for further research. Likewise, a favourable outcome amongst HPV+ tumours may raise questions about new strategies for organ preservation [10]. Clearly, the response to these questions must be addressed in the analysis of larger data sets of HPV+ tumours. Also, due to small sample size, the relevance of fractionation in HPV+ tumours cannot be addressed in the present study. Conversely, however, more insight can be gained regarding HPV− tumours, which represented the majority of the analysed cases. Figure 3 illustrates that loco-regional control in HPV− tumours was improved by p-CAIR, but the difference did not appear to be significant (p = 0.37). The qualitative outcome of the trial in the HPV− subset appeared, thus, similar to that obtained in a whole data set of 279 patients [7].
An interesting observation was the detection of two metachronous malignant tumours amongst nine individuals with HPV+ tumours. The rate of synchronous and metachronous lesions in HPV-positive SCCHN is, at present, largely unknown. Some case reports suggest increased susceptibility of patients with HPV+ tumours to synchronous tumours [11, 12]. Other studies suggest, however, lower incidence of metachronous tumours in HPV+ cases [13].
HPV infection versus expression of selected molecular markers
Several studies have shown overexpression of p16 in HPV+ tumours, and some of them suggested the potential role of this marker as a surrogate for HPV infection [14, 15]. The relationship between HPV infection and expression of the other markers has been also investigated in these studies. While a small number of HPV+ tumours in the present data set preclude statistically meaningful conclusions, the analysis supports studies showing that HPV infection is associated with low expression of EGFR and cyclin D in tumour cells [14, 15]. Differences in expression of molecular markers in HPV+ and HPV− tumours provide additional support for the existence of two distinct carcinogenetic pathways for the development of HNSCC: one driven by carcinogenic effects of tobacco or alcohol and another by HPV-induced cell cycle dysregulation.
References
Ang KK, Harris J, Wheeler R et al (2010) Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med 363:24–35
Ragin CC, Taioli E (2007) Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: review and meta-analysis. Int J Cancer 121:1813–1820
Fakhry C, Westra WH, Li S et al (2008) Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst 100:261–269
Vidal L, Gillison LV (2008) Human papillomavirus in HNSCC: recognition of a distinct disease type. Hematol Oncol Clin N Am 22:1125–1142
Kreimer AR, Clifford GM, Boyle P, Franceschi S (2005) Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev 14:467–475
Marur S, D’Souza G, Westra WH, Forastiere AA (2010) HPV-associated head and neck cancer: a virus-related cancer epidemic. Lancet Oncol [Epub ahead of print]
Suwinski R, Bankowska-Wozniak M, Majewski W et al (2008) Randomized clinical trial on 7-days-a-week postoperative radiotherapy for high-risk squamous cell head and neck cancer. Radiother Oncol 87:155–163
Suwinski R, Jaworska M, Nikiel B et al (2010) Predicting the effect of accelerated fractionation in postoperative radiotherapy for head and neck cancer based on molecular marker profiles: data from a randomized clinical trial. Int J Radiat Oncol Biol Phys 77:438–446
Heck JE, Berthiller J, Vaccarella S et al (2010) Sexual behaviours and the risk of head and neck cancers: a pooled analysis in the International Head and Neck Cancer Epidemiology (INHANCE) consortium. Int J Epidemiol 39:166–181
Worden FP, Kumar B, Lee JS et al (2008) Chemoselection as a strategy for organ preservation in advanced oropharynx cancer: response and survival positively associated with HPV16 copy number. J Clin Oncol 26:3138–3146
McGovern SL, Williams MD, Weber RS et al (2009) Three synchronous HPV-associated squamous cell carcinomas of Waldeyer’s ring: Case report and comparison with Slaughter’s model of field cancerization. Head Neck [Epub ahead of print]
Han TJ, Lee CH, Yoo CW et al (2009) Synchronous multifocal HPV-related neoplasm involving both the genital tract and the head-and-neck area: a case report of Fanconi anemia. Radiother Oncol 92:138–141
Licitra L, Perrone F, Bossi P et al (2006) High-risk human papillomavirus affects prognosis in patients with surgically treated oropharyngeal squamous cell carcinoma. J Clin Oncol 24:5630–5636
Reimers N, Kasper HU, Weissenborn SJ et al (2007) Combined analysis of HPV-DNA, p16 and EGFR expression to predict prognosis in oropharyngeal cancer. Int J Cancer 120:1731–1738
Hafkamp HC, Speel EJ, Haesevoets A et al (2003) A subset of head and neck squamous cell carcinomas exhibits integration of HPV16/18 DNA and overexpression of p161NK4A and p53 in the absence of mutations in p53 exons 5–8. Int J Cancer 107:394–400
Acknowledgments
This research was supported by research grant MN 402 108 134 provided by the Polish Ministry of Science and Higher Education. The data were presented at the Fourth European Congress on Head and Neck Oncology 2010, Athens, Greece.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Snietura, M., Piglowski, W., Jaworska, M. et al. Impact of HPV infection on the clinical outcome of p-CAIR trial in head and neck cancer. Eur Arch Otorhinolaryngol 268, 721–726 (2011). https://doi.org/10.1007/s00405-010-1396-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-010-1396-7