
Abstract
Background
Reverse shoulder arthroplasty (RSA) has shown promising results for cuff tear arthropathy but the indication has been extended to fracture sequelae and revision shoulder arthroplasty with different preconditions. Further, the clinical relevance of inferior scapular notching for different etiologies is uncertain. Our hypothesis was that preoperative etiology as well as the occurrence of scapular notching would significantly influence the clinical outcome.
Methods
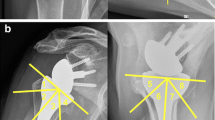
We reviewed 76 reverse shoulder arthroplasties for cuff tear arthropathy (45 patients), fracture sequelae (10 patients) and revision arthroplasty (21 patients) retrospectively. The follow-up consisted of 71 patients and the mean follow-up period was 23 months (±14 months). All patients were evaluated postoperatively using the Constant score adjusted for age and gender and the simple shoulder test. A radiological investigation was performed preoperatively and at the time of the final follow-up including the evaluation of scapular notching according to Sirveaux. For further evaluation of scapular notching, patients were separated into three groups according to the inferior glenosphere overlap: negative or no inferior overlap −6–0 mm), mild overlap (1–4 mm) and pronounced overlap (5–9 mm).
Results
After a mean follow-up of 23 months the average age- and gender-adjusted Constant score (CS) was 77.8 % (±26 %). According to the etiology, patients with cuff tear arthropathy (CTA) showed a higher CS of 83 % compared with patients with fracture sequelae (CS 73 %) and compared with patients who had undergone RSA as a revision for failed shoulder arthroplasty (CS 69 %). The difference was significant comparing the cuff tear arthropathy patients with the revision surgery patients (p = 0.035). Within the group of fracture sequelae, patients with type three sequelae according to the Boileau classification (surgical neck nonunion) had a significantly worse outcome compared with the type four fracture sequelae patients (severe tuberosity dislocation) (CS 57 vs. 87 %, p = 0.01). The overall complication rate was 27 % with 8 % infections and 9 % dislocations. Revision surgery was necessary in 11.5 % with removal or replacement of the implants in 8 %. Inferior scapular notching was detected in 43 % of the patients. These patients had an inferior CS (70 ± 18 %) compared with patients without scapular notching (84 ± 25 %, p = 0.015). The incidence of scapular notching was significantly reduced with an increasing inferior overlap of the glenosphere.
Conclusions
In conclusion, we found the preoperative etiology to influence the clinical results after RSA with superior results given for cuff tear arthropathy and inferior results for revision arthroplasty and fracture sequelae type three. Further, we found a correlation between scapular notching and the clinical outcome. The inferior scapular notching was significantly reduced by an increased inferior glenosphere overlap.
Level of evidence
Level IV, case series, treatment study.





Similar content being viewed by others


References
Boileau P, Trojani C, Walch G, Krishnan SG, Romeo A, Sinnerton R (2001) Shoulder arthroplasty for the treatment of the sequelae of fractures of the proximal humerus. J Should Elb Surg 10(4):299–308. doi:10.1067/mse.2001.115985
Boileau P, Watkinson D, Hatzidakis AM, Hovorka I (2006) Neer Award 2005: the Grammont reverse shoulder prosthesis: results in cuff tear arthritis, fracture sequelae, and revision arthroplasty. J Should Elb Surg 15(5):527–540. doi:10.1016/j.jse.2006.01.003
Boileau P, Watkinson DJ, Hatzidakis AM, Balg F (2005) Grammont reverse prosthesis: design, rationale, and biomechanics. J Should Elb Surg 1(Suppl S):147S–161S
Grammont PM, Baulot E (1993) Delta shoulder prosthesis for rotator cuff rupture. Orthopedics 16(1):65–68
Grammont PM, Baulot E (2011) The classic: delta shoulder prosthesis for rotator cuff rupture. 1993. Clin Orthop Relat Res 469(9):2424. doi:10.1007/s11999-011-1960-5
Gutierrez S, Levy JC, Frankle MA, Cuff D, Keller TS, Pupello DR et al (2008) Evaluation of abduction range of motion and avoidance of inferior scapular impingement in a reverse shoulder model. J Should Elb Surg 17(4):608–615
Hamada K, Fukuda H, Mikasa M, Kobayashi Y (1990) Roentgenographic findings in massive rotator cuff tears. A long-term observation. Clin Orthop Relat Res 254:92–96
Kappe T, Cakir B, Reichel H, Elsharkawi M (2011) Reliability of radiologic classification for cuff tear arthropathy. J Should Elb Surg 20(4):543–547. doi:10.1016/j.jse.2011.01.012
Kelly JD 2nd, Zhao JX, Hobgood ER, Norris TR et al (2012) Clinical results of revision shoulder arthroplasty using the reverse prosthesis. J Should Elb Surg. doi:10.1016/j.jse.2011.11.021
Levigne C, Boileau P, Farvard L, Garaud P, Mole D, Sirveaux F et al (2006) Scapular notching in reverse shoulder arthroplasty. In: Walch G, Boileau P, Molé D (eds) Reverse shoulder arthroplasty: clinical results, complications, revision. Montpellier: Sauramps medical, pp 353–372
Simovitch RW, Zumstein MA, Lohri E, Helmy N, Gerber C (2007) Predictors of scapular notching in patients managed with the Delta III reverse total shoulder replacement. J Bone Joint Surg Am 89(3):588–600. doi:10.2106/JBJS.F.00226
Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Mole D (2004) Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J Bone Joint Surg Br 86(3):388–395
Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Molé D (2004) Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J Bone Joint Surg Br 86(3):388–395
Stechel A, Fuhrmann U, Irlenbusch L, Rott O, Irlenbusch U (2010) Reversed shoulder arthroplasty in cuff tear arthritis, fracture sequelae, and revision arthroplasty. Acta Orthop 81(3):367–372. doi:10.3109/17453674.2010.487242
Walker M, Willis MP, Brooks JP, Pupello D, Mulieri PJ, Frankle MA (2012) The use of the reverse shoulder arthroplasty for treatment of failed total shoulder arthroplasty. J Should Elb Surg 21(4):514–522. doi:10.1016/j.jse.2011.03.006
Wall B, Nove-Josserand L, O’Connor DP, Edwards TB, Walch G (2007) Reverse total shoulder arthroplasty: a review of results according to etiology. J Bone Joint Surg Am 89(7):1476–1485
Werner CM, Steinmann PA, Gilbart M, Gerber C (2005) Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 87(7):1476–1486
Willis M, Min W, Brooks JP, Mulieri P, Walker M, Pupello D et al (2012) Proximal humeral malunion treated with reverse shoulder arthroplasty. J Should Elb Surg 21(4):507–513. doi:10.1016/j.jse.2011.01.042
Conflict of interest
The authors, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article. The author declares nofinancial bias.
Ethical approval
The approval of the Ethical Committee of the Hanover Medical School was given by the director Prof. Dr. H.D. Tröger in April 15, 2010; the study number is 814.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wellmann, M., Struck, M., Pastor, M.F. et al. Short and midterm results of reverse shoulder arthroplasty according to the preoperative etiology. Arch Orthop Trauma Surg 133, 463–471 (2013). https://doi.org/10.1007/s00402-013-1688-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-013-1688-7